False Logic Explanations For 5 Techniques Inoculating Against
Myths Debunked 9 Myths 10 Myths Busted Myths Explained
History of Antivax Movements Facts and Myths
Denialist Fallacies 41 Covid Myths ?

In the psychology of human behavior, denialism is a person's choice to deny reality as a way to avoid a psychologically uncomfortable truth. Denialism is an essentially irrational action that withholds the validation of a historical experience or event, when a person refuses to accept an empirically verifiable reality.
In the sciences, denialism is the rejection of basic facts and concepts that are undisputed, well-supported parts of the scientific consensus on a subject, in favor of radical and controversial ideas.
The motivations and causes of denialism include religion, self-interest (economic, political, or financial), and defence mechanisms meant to protect the psyche of the denialist against mentally disturbing facts and ideas.
https://en.wikipedia.org/wiki/Denialism
Manufactroversy

Mechanisms of manufacturing controversy and uncertainty
Manufacturing controversy has been a tactic used by ideological and corporate groups in order to "neutralize the influence of academic scientists" in public policy debates. Cherry picking of favorable data and sympathetic experts, aggrandizement of uncertainties within theoretical models, and false balance in media reporting contribute to the generation of manufactured controversies.
The formula is to amplify uncertainties, cherry-pick experts, attack individual scientists, marginalize the traditional role of distinguished scientific bodies and get the media to report "both sides" of a manufactured controversy.
Those manufacturing uncertainty may label academic research as "junk science" and use a variety of tactics designed to stall and increase the expense of the distribution of sound scientific information. Delay tactics are also used to slow the implementation of regulations and public warnings in response to previously undiscovered health risks (e.g., the increased risk of Reye's syndrome in children who take aspirin). Chief among these stalling tactics is generating scientific uncertainty, "no matter how powerful or conclusive the evidence", in order to prevent regulation.
Another tactic used to manufacture controversy is to cast the scientific community as intolerant of dissent and conspiratorially aligned with industries or sociopolitical movements that quash challenges to conventional wisdom. This form of manufactured controversy has been utilized by environmentalist advocacy groups, religious challengers of the theory of evolution, and opponents of global warming legislation.
https://en.wikipedia.org/wiki/Manufactured_controversy

Two Tactics - Effectively Limit the Spread of Science Denialism
https://arstechnica.com/science/2019/06/debunking-science-denialism-does-work-but-not-perfectly/
- Doubt the Science
- Question Scientists’ Motives and Integrity
- Magnify Disagreements among Scientists and Cite Gadflies as Authorities
- Exaggerate Potential Harm
- Appeal to Personal Freedom
- Reject Whatever Would Repudiate A Key Philosophy
The purpose of the denialism playbook is to advance rhetorical arguments that give the appearance of legitimate debate when there is none. My purpose here is to penetrate that rhetorical fog, and to show that these are the predictable tactics of those clinging to an untenable position. If we hope to find any cure for (or vaccine against) science denialism, scientists, journalists and the public need to be able recognize, understand and anticipate these plays.
To illustrate how the playbook works—and sadly, it is very effective –I will break down the chiropractor and creationist versions, which have endured for many decades in spite of overwhelming evidence, and point out parallels to the coronavirus rhetoric.
THE PLAYBOOK
1. Doubt the Science
The first tactic of denialism is to raise objections to scientific evidence or interpretations. This may take the form of seemingly legitimate specific arguments against a scientific claim. For example, chiropractors sought other explanations besides vaccine efficacy to account for the decline of infectious diseases: “The Center for Disease Control statistics make it clear that the majority of diseases that are now routinely vaccinated against were disappearing before either the cause was discovered or the vaccine developed,” stated a 1995 letter to the editor of Dynamic Chiropractic magazine. In polio’s case, this argument does not hold up against the facts that: (a) the disease was surging in the 1950s; (b) the vaccine was proven effective in a massive double-blind, placebo-controlled trial; and (c) infections declined precipitously after the introduction of the vaccine.
Alternatively, some statements are blanket arguments against an entire scientific discipline. For example, Henry Morris, whose 1961 book The Genesis Flood is credited with reviving the creationism movement, alleged: “Since there is no real scientific evidence that evolution is occurring at present or ever occurred in the past, it is reasonable to conclude that evolution is not a fact of science, as many claim. In fact, it is not even science at all, but an arbitrary system built upon faith in universal naturalism.”
2. Question Scientists’ Motives and Integrity
As a growing body of consistent evidence can be hard to explain away, one fallback is to impugn the source. In the vaccination arena, this often takes the form of alleging financial conflicts of interest on the part of scientists, greed on the part of manufacturers, and complicity of government officials. “It appears that the scientific foundation on which these vaccines have been erected is fragile enough that only compulsory laws, expensive public relations efforts, outrageous propaganda, and expensive advertising must ensue for compliance to be maintained,” wrote one author in American Chiropractor. Salk, by the way, filed no patent.
In the evolution arena, scientists are often accused of being part of a conspiracy to undermine religion through educational systems. Kenneth Cumming, of the Institute for Creation Research, objected to a PBS series on evolution by drawing a parallel to the 9/11 attackers: “America is being attacked from within through its public schools by a militant religious movement of philosophical naturalists (i.e., atheists) under the guise of secular Darwinism. Both desire to alter the life and thinking of our nation.” One noteworthy counter to such assertions is the Clergy Letter Project, which has gained the support of more than 15,000 Christian clergy for the teaching of evolution.
3. Magnify Disagreements among Scientists and Cite Gadflies as Authorities
In all scientific arenas, there is honest disagreement about the interpretation of evidence. However, these differences are deliberately inflated by denialists to imply a lack of consensus on more fundamental points, while often propounding the contradictory views of a few unqualified outliers. An example of the latter is how some chiropractors have seized on the anti-vaccination stance of one critic, Viera Scheibner. Her claim that there is no evidence for vaccine efficacy or safety is cited repeatedly, while overlooking the fact that her training and expertise is in geology, not medicine.
In the evolution arena, differences of interpretation among scientists are relished by antievolution voices. For example, the initial discovery of a new fossil hominid usually elicits some different interpretations and expressions of uncertainty in the scientific community. Creationists often mischaracterize these normal dynamics of scientific discourse as “skepticism” over the significance of such finds so as to discount them. By overblowing legitimate disagreements and propounding “alternatives” to evolution, denialists often make appeals to “teach the controversy,” when no such controversy exists in the scientific community. Different interpretations of a fossil do not negate the discomfiting evidence for the antiquity of human ancestors.
Antievolution leaders in the U.S. also include a small number of scholars whose credentials are in other disciplines. For example, the abovementioned Henry Morris was an engineer, not a biologist. Phillip E. Johnson, whose book Darwin on Trial inspired many adherents to the intelligent design movement, was a law professor with no formal training in biology.
A lack of credentials or status within the scientific community is often seen not as a liability but as a virtue. Scientists Pascal Diethelm and Martin McKee note, “Denialists are usually not deterred by the extreme isolation of their theories, but rather see it as the indication of their intellectual courage against the dominant orthodoxy and the accompanying political correctness, often comparing themselves to Galileo.”
4. Exaggerate Potential Harm
When the evidence contradicts a position, another recourse is to try to incite fear. No vaccine or medicine is 100 percent safe, without any risk of side effects. Chiropractors have long emphasized the potential side effects of vaccines, for example in a statement in Dynamic Chiropractic offering a litant of possible effects: “death, encephalopathy, demyelinating diseases, brachial neuritis, Guillain-Barré syndrome, infections generated by vaccine agents, anaphylaxis, subacute sclerosing panencephalitis, seizure disorder, optic neuritis, arthritis,” and so on. However, they generally fail to acknowledge the serious consequences of infections that would be prevented by vaccination.
But what harm could arise from knowing a bit about evolution? Well, Hitler, of course! “Of the many factors that produced the Nazi Holocaust and World War II,” wrote one critic in the Journal of Creation, “one of the most important was Darwin’s notion that evolutionary progress occurs mainly as a result of the elimination of the weak in the struggle for survival.” It is an oft-repeated argument that has no bearing of course on the veracity of Darwin’s theory.
Vaccination foes have lobbed similar accusations, likening physicians who administer vaccines to Nazi doctors and alleging that vaccines violate the 1947 Nuremberg Code of medical ethics.
5. Appeal to Personal Freedom
If fear is not persuasive, there is another fallback position that resonates strongly with Americans: the freedom of choice. The American Chiropractic Association leaned on this cherished notion when it established its official vaccination policy:
“Since the scientific community acknowledges that the use of vaccines is not without risk, the American Chiropractic Association supports each individual’s right to freedom of choice in his/her own health care based on an informed awareness of the benefits and possible adverse effects of vaccination. The ACA is supportive of a conscience clause or waiver in compulsory vaccination laws… providing an elective course of action regarding vaccination.”
Likewise, the International Chiropractic Association “questions the wisdom of mass vaccination programs” and views compulsory programs as an infringement of “the individual’s right to freedom of choice.”
Similarly, the teaching of evolution in public schools is viewed as an assault upon the religious freedom of those who oppose it. Those holding this view advocate for disclaimers on textbooks (“just a theory”), the teaching of “alternative” views of the history of life (Genesis or intelligent design), or the freedom to opt out of the evolution curriculum of biology classes.
Notably, the U.S. Supreme Court has rejected challenges to compulsory vaccination partly on the grounds that individual belief cannot subordinate the safety of an entire community. And U.S. courts have repeatedly struck down attempts to subvert the teaching of evolution as religiously motivated and violations of the establishment clause of the First Amendment of the U.S. Constitution.
6. Reject Whatever Would Repudiate a Key Philosophy
Once the courts have spoken, and the scientific evidence grows to be overwhelming, one might think that denialists would be out of plays. But there is one last line of defense that reveals the nucleus of denial: It is not that some scientific claim is untrue; it is that it is unacceptable in light of some philosophical commitment. The science must be summarily rejected.
Chiropractic was founded in the early 20th century on the assertion that all disease has its origins in misalignments of the spine. “Chiropractors have found in every disease that is supposed to be contagious, a cause in the spine,” claimed Bartlett Joshua Palmer, the son of chiropractic founder Daniel David Palmer. Acceptance of germ theory and vaccination would repudiate the founding premise of the profession that all disease stems from vertebral misalignments. Therefore, that premise cannot be questioned.
With respect to evolution, Henry Morris made it plain: “When science and the Bible differ, science has obviously misinterpreted its data.”
Any credence granted to evolutionary science is a threat to a worldview based on interpretation of the Bible; David Cloud, a publisher of Bible study materials argues: “If the Bible does not mean what it says, there is no way to know what it does mean.
Historian of science and author Naomi Oreskes has coined a term for this stance: “implicatory denial”—the rejection of scientific findings because we don’t like their implications.
As these positions are reinforced by family or community, they harden into part of one’s identity. “In this way, cultural identity starts to override facts,” Norwegian climate psychologist Per Espen Stoknes has said. “And my identity trumps truth any day.”
Psychologists Elliot Aronson and Carol Tavris write in the Atlantic: “[W]hen people feel a strong connection to a political party, leader, ideology, or belief, they are more likely to let that allegiance do their thinking for them and distort or ignore the evidence that challenges those loyalties.”
The denialist playbook is now erupting around the coronavirus. Although COVID-19 is new, the reactions to public health measures, scientific claims, and expert advice are not. Attitudes and behaviors concerning the threat posed by the coronavirus (doubting the science), the efficacy of lockdowns and mask wearing (freedoms being eroded) and alternative treatments (gadflies over experts) are being driven as much or more by rhetoric than by evidence.
Polls indicate that despite the devastating health and economic impacts of the pandemic, with respect to a potential vaccine we are nowhere near as united as Americans were in 1955. But as epidemiologist Michael Osterholm noted in June, “Eventually there won't be any blue states or red states. There won't be any blue cities or red rural areas. It'll all be COVID colored.”
Now, sadly, there is no denying that.
The Denialist Playbook - Sean B. Carroll
https://www.scientificamerican.com/article/the-denialist-playbook/
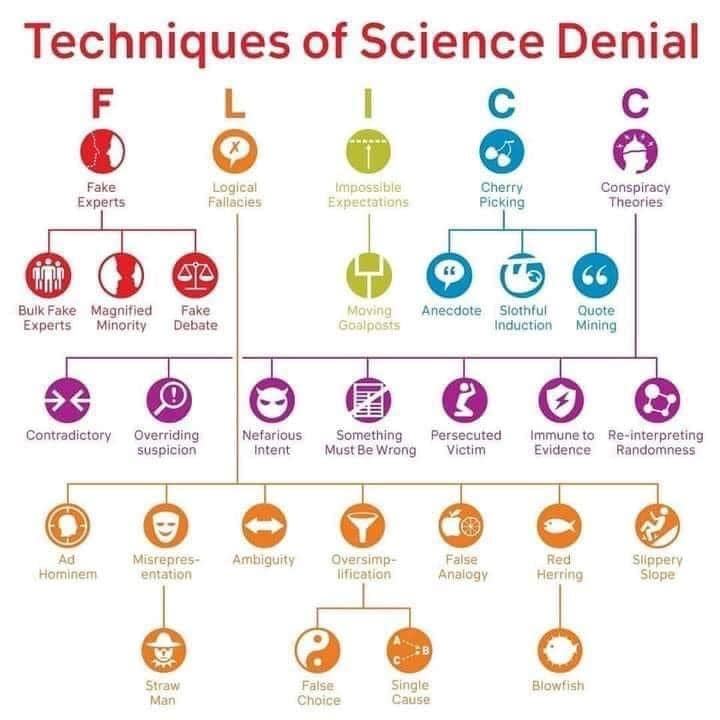
15 Science Denialist Tactics | Debunking Denialism
Fake Experts
Because pseudoscience is not supported by the bulk of scientific evidence, science denialists need to rely on fake experts to push their nonsense. These do not have the required relevant scientific background or research experience to be trusted. Read more about fake experts.
False Balance
Since pseudoscience is not based on evidence, science denialists need to make it appear as if they represents a different, yet equally valid, approach to reality. This is done by demanding that equal treatment be given to both science and pseudoscience. Read more about false balance.
Conspiratorial Thinking
In order to explain away the massive amount of scientific evidence contradicting their pseudoscience, science denialists have to invent conspiracy theories of why the establishment is conspiring together to hide the truths. Read more about conspiratorial thinking.
Distorting Quotes
Pseudoscience is an imposter of science. Therefore, science denialists need to take quotes by real scientists and distort them or take them out of context so that they superficially seem to support pseudoscientific claims. Read more about distorting quotes.
Merchants of Doubt
Science denialists often attack scientists who publish inconvenient research. This is done by funding NGOs, harassing scientists with spam requests for emails, distorting those communications and sending the package to an ignorant or sympathetic journalist. These journalists then write misleading hit pieces on the scientist in an effort to undermine their credibility.
Selective Skepticism
Selective skepticism is used by pseudoscience activists to applying enormous and harsh skepticism against evidence that contradicts their beliefs, while exposing data that superficially supports their claims to virtually no critical analysis.
Cherry Picking
In order to create the illusion of scientific supports, science denialists must pick out those few anomalous studies that appear to support their beliefs while ignoring the bulk of scientific evidence showing that they are wrong. This form of cherry picking distorts the scientific knowledge mass in a deceptive way.
Moving the Goalposts
Since pseudoscience activists want keep believing nonsense, they must continue to demand more and more evidence and never be satisfied. By erecting these impossible expectations, science denialists can move the goalposts again and again and never have to give up their position.
Obfuscating Basic Science
Many anti-science activists are often ignorant about basic scientific facts about issues they discuss, so they push simple misunderstandings about definitions, mechanism, arguments and evidence.
Anomaly Hunting
Because science denialists cannot defeat scientific explanations, they put extreme focus on one or a few tiny details that are unexplained and try to claim that this undermines the entire scientific knowledge mass in that area.
Confusing Mechanism With Fact
Another common tactic is to attempt to spread uncertainty and doubt about a scientific fact by questioning some aspect of the proposed mechanism, which may be less researched that the scientific fact itself. By confusing mechanism with fact, science denialists work to undermine confidence in well-established scientific facts.
Manufactroversy
One way to attack the massive amount of scientific evidence for mainstream scientific models is to insist that there is a scientific controversy where there really isn’t one. By portraying the situation as a controversy, science denialists can make it appear as if it is reasonable tor reject mainstream science.
Playing the Martyr Card
Because science denialist almost never get traction with the scientific community, they must explain this somehow. The typical way they do this is to compare themselves with Einstein or Galileo and insist that they are oppressed martyrs. But not all rebels and mavericks are budding scientific revolutionaries. Some are just mavericks.
Blowing Honest Errors out of Proportion
Scientists sometimes make honest errors. Pseudoscience activists love to blow these errors out of proportion, and make it look like a small error in some details is somehow a major error about larger issues in a specific scientific field.
Gish Gallop
The Gish Gallop involves spewing a torrent of as many bad and unscientific claims as possible in a short amount of time to overwhelm any science advocate and make it difficult to counter all of the misinformation. Named after the young earth creationist Duane Gish who often used this tactic when debating scientists on evolution.
https://debunkingdenialism.com/critical-thinking/science-denialist-tactics/
The False Logic behind Science Denial
Those who argue that COVID-19 isn’t a real threat are mirroring bogus attacks on global warming and evolution

Climate change: I reject the suggestion that the “magic of the market” has failed and that we need government intervention to remedy the market failure. Evolutionary theory: I am offended by the suggestion that life is random and meaningless and that there is no God. COVID-19: I resent staying home, losing income or being told by the government what do to.
In many cases, these objections are based on misunderstandings; evolutionary theory does not prove the nonexistence of God. In others, the implications are real enough. Climate change is a market failure, which will take government action to address. And absent a system for widespread testing and contact tracing, there was no known way to slow the spread of SARS-CoV-2 in the U.S. without the majority of us staying home. COVID-19 has shown how dangerous the fallacy of implicatory denial is. When we reject evidence because we do not like what it implies, we put ourselves at risk.
The U.S. could have acted more quickly to contain COVID-19. If we had, we would have saved both lives and jobs. But facts have an inconvenient habit of getting in the way of our desires. Sooner or later, denial crashes on the rocks of reality. The only question is whether it crashes before or after we get out of the way.
The False Logic behind Science Denial - Scientific American
https://www.scientificamerican.com/article/the-false-logic-behind-science-denial/
Sociological explanations for climate change denial - Resilience
Ron Kramer, a sociologist at Western Michigan University, has been studying how sociological and cultural factors are preventing Americans from talking about or acting on climate change. He drew on the research of sociologist Stanley Cohen, professor emeritus at the London School of Economics, who says that denial “refers to the maintenance of social worlds in which an undesirable situation (event, condition, phenomenon) is unrecognized, ignored or made to seem normal.”
He cites three categories of denial:
- A literal denial is: “the assertion that something did not happen or is not true.”
- With an interpretive denial, the basic facts are not denied, however, “…they are given a different meaning from what seems apparent to others.” People recognize that something is happening but that it’s good for us.
- Implicatory denial “covers the multitude of vocabularies, justifications, rationalizations, evasions that we use to deal with our awareness of so many images of unmitigated suffering.” Here, “knowledge itself is not an issue. The genuine challenge is doing the ‘right’ thing with this knowledge.”
Through literal and interpretive denial, climate change deniers declare that the earth is not warming even though 98 percent of our scientists have written thousands of peer-reviewed papers and reports concluding that climate change is real and caused by human activity…
…In implicatory denial people recognize that something untoward is happening but they fail to act because they are emotionally uncomfortable or troubled about it…
Sociological explanations for climate change denial - Resilience
https://www.resilience.org/stories/2012-03-17/sociological-explanations-climate-change-denial/
The 5 Telltale Techniques of Climate Change Denial
CNN — There is overwhelming scientific evidence that humans are causing global warming. Nevertheless, a small proportion of the population continues to deny the science. This can be problematic when the small number denying climate science includes half of the U.S. Senate.
How do you identify climate science denial, and how do you respond to it? To address denial properly, you need to understand the telltale techniques used to distort the science. It turns out all movements that deny a scientific consensus, whether it be the science of climate change, evolution or vaccination, share five characteristics in common:
1. Fake experts
Ninety-seven percent of climate scientists agree that humans are causing global warming. This has been found independently in a number of studies, including surveys of Earth scientists, analysis of public statements about climate change and analysis of peer-reviewed scientific papers. How might one cast doubt on the overwhelming scientific consensus? One technique is the use of fake experts.
We see this in online petitions such as the Global Warming Petition Project, which features more than 31,000 scientists claiming humans aren’t disrupting our climate. How can there be 97% consensus when 31,000 scientists disagree? It turns out 99.9% of the petition’s signatories aren’t climate scientists. They include computer scientists, mechanical engineers and medical scientists but few climate scientists. The Global Warming Petition Project is fake experts in bulk.
2. Logical fallacies
The reason why there’s a 97% consensus is because of the many lines of evidence that humans are causing global warming. Human fingerprints are being observed in heat escaping out to space, in the structure of the atmosphere and even in the changing seasons. Another denialist technique used to counter the weight of evidence is the logical fallacy.
The most common fallacious argument is that current climate change must be natural because climate has changed naturally in the past. This myth commits the logical fallacy of jumping to conclusions. It’s like finding a dead body with a knife sticking out of its back, and arguing that the person must have died of natural causes because humans have died of natural causes in the past. The premise does not lead to the conclusion.
3. Impossible expectations
While many lines of evidence inform our understanding of climate change, another source of understanding are climate models. These are computer simulations built from the fundamental laws of physics, and they have made many accurate predictions since the 1970s. Climate models have successfully predicted the loss of Arctic sea ice, sea level rise and the geographic pattern of global warming. However, one technique used to cast doubt on climate models is the tactic of impossible expectations.
Some people argue that climate models are unreliable if they don’t make perfect short-term predictions. However, a number of unpredictable influences such as ocean and solar cycles have short-term influences on climate. Over the long term, these effects average out, which is why climate models do so well at long-term predictions.
4. Cherry-picking
Signs of global warming have been observed all over our planet. Ice sheets in Greenland and Antarctica are losing hundreds of billions of tons of ice every year. Global sea level is rising. Thousands of species are migrating toward cooler regions in response to warming. The ocean is building up four atomic bombs worth of heat every second. One way to avoid this overwhelming body of evidence is through the technique of cherry-picking.
For example, a persistent myth is that global warming stopped in recent decades. This is done by focusing on one slice of our climate system – the surface temperature record. Further, it relies on cherry-picking short time periods. This ignores the long-term trend and more importantly, ignores the many warming indicators telling us that our planet continues to build up heat.
5. Conspiracy theory
The global surface temperature record is constructed by teams across the world, each compiling their own independent record. These different efforts, each using their own methods, paint a consistent picture of global warming. Climate science deniers reject this coherent evidence with conspiracy theories.
The thousands of scientists across the world who develop these temperature records are regularly accused of faking their data to inflate the global warming trend. Of course, critics produce no evidence for a global conspiracy. In fact, a number of investigations into the scientists’ methodology has concluded that they conducted their research with robust integrity. How do the conspiracy theorists respond to each exoneration? By expanding their conspiracy theory to include the investigators!
The link between conspiratorial thinking and science denial has serious and practical consequences. Conspiracy theorists are immune to scientific evidence, as any evidence conflicting with their beliefs is considered part of a conspiracy. The implication is that the most effective approach is not changing the mind of the unchangeable. Rather a more fruitful approach is communicating the realities of climate change to the large, undecided majority who are open to scientific evidence. A crucial part of the puzzle is explaining the techniques of science denial. This has the powerful effect of inoculating people against the misinformation of climate science deniers.
The 5 telltale techniques of climate change denial
https://www.cnn.com/2015/07/22/opinions/cook-techniques-climate-change-denial/index.html
Inoculating Against Science Denial
Science denial has real, societal consequences. Denial of the link between HIV and AIDS led to more than 330,000 premature deaths in South Africa. Denial of the link between smoking and cancer has caused millions of premature deaths. Thanks to vaccination denial, preventable diseases are making a comeback.
Denial is not something we can ignore or, well, deny. So what does scientific research say is the most effective response? Common wisdom says that communicating more science should be the solution. But a growing body of evidence indicates that this approach can actually backfire, reinforcing people’s prior beliefs.
When you present evidence that threatens a person’s worldview, it can actually strengthen their beliefs. This is called the “worldview backfire effect”. One of the first scientific experiments that observed this effect dates back to 1975.
A psychologist from the University of Kansas presented evidence to teenage Christians that Jesus Christ did not come back from the dead. Now, the evidence wasn’t genuine; it was created for the experiment to see how the participants would react.
Transparent, research-based, written by experts – and always free.
About us
What happened was their faith actually strengthened in response to evidence challenging their faith. This type of reaction happens across a range of issues. When US Republicans are given evidence of no weapons of mass destruction in Iraq, they believe more strongly that there were weapons of mass destruction in Iraq. When you debunk the myth linking vaccination to autism, anti-vaxxers respond by opposing vaccination more strongly.
In my own research, when I’ve informed strong political conservatives that there’s a scientific consensus that humans are causing global warming, they become less accepting that humans are causing climate change.
Brute force meets resistance
Ironically, the practice of throwing more science at science denial ignores the social science research into denial. You can’t adequately address this issue without considering the root cause: personal beliefs and ideology driving the rejection of scientific evidence. Attempts at science communication that ignore the potent influence effect of worldview can be futile or even counterproductive.
How then should scientists respond to science denial? The answer lies in a branch of psychology dating back to the 1960s known as “inoculation theory”. Inoculation is an idea that changed history: stop a virus from spreading by exposing people to a weak form of the virus. This simple concept has saved millions of lives.
In the psychological domain, inoculation theory applies the concept of inoculation to knowledge. When we teach science, we typically restrict ourselves to just explaining the science. This is like giving people vitamins. We’re providing the information required for a healthier understanding. But vitamins don’t necessarily grant immunity against a virus.
There is a similar dynamic with misinformation. You might have a healthy understanding of the science. But if you encounter a myth that distorts the science, you’re confronted with a conflict between the science and the myth. If you don’t understand the technique used to distort the science, you have no way to resolve that conflict.
Half a century of research into inoculation theory has found that the way to neutralise misinformation is to expose people to a weak form of the misinformation. The way to achieve this is to explain the fallacy employed by the myth. Once people understand the techniques used to distort the science, they can reconcile the myth with the fact.

Skeptical Science
There is perhaps no more apt way to demonstrate inoculation theory than to address a myth about vaccination. A persistent myth about vaccination is that it causes autism.
This myth originated from a Lancet study which was subsequently shown to be fraudulent and was retracted by the journal. Nevertheless, the myth persists simply due to the persuasive fact that some children have developed autism around the same time they were vaccinated.
This myth uses the logical fallacy of post hoc, ergo propter hoc, Latin for “after this, therefore because of this”. This is a fallacy because correlation does not imply causation. Just because one event happens around the same time as another event doesn’t imply that one causes the other.
The only way to demonstrate causation is through statistically rigorous scientific research. Many studies have investigated this issue and shown conclusively that there is no link between vaccination and autism.
Inoculating minds
The response to science denial is not just more science. We stop science denial by exposing people to a weak form of science denial. We need to inoculate minds against misinformation.
The practical application of inoculation theory is already happening in classrooms, with educators adopting the teaching approach of misconception-based learning (also known as agnotology-based learning or refutational teaching).
This involves teaching science by debunking misconceptions about the science. This approach results in significantly higher learning gains than customary lectures that simply teach the science.
While this is currently happening in a few classrooms, Massive Open Online Courses (or MOOCs) offer the opportunity to scale up this teaching approach to reach potentially hundreds of thousands of students. At the University of Queensland, we’re launching a MOOC that makes sense of climate science denial.
Our approach draws upon inoculation theory, educational research into misconception-based learning and the cognitive psychology of debunking. We explain the psychological research into why and how people deny climate science.
Having laid the framework, we examine the fallacies behind the most common climate myths. Our goal is for students to learn how to identify the techniques used to distort climate science and feel confident responding to misinformation.
A typical response of scientists to science denial is to teach more science. But that only provides half of what’s needed. Scientific research has offered us a solution: build resistance to science denial by exposing people to a weak form of science denial.
Inoculating against science denial
https://theconversation.com/inoculating-against-science-denial-40465
Articles on Science Denial – News, Research and Analysis
https://theconversation.com/us/topics/science-denial-16371
The Use of Denialist Tactics to Confuse Scientific Knowledge
https://scienceblogs.com/author/denialism
Vaccine Myths Debunked | PublicHealth.org
U.S. public health officials and physicians have been combating misconceptions about vaccine safety for over twenty years. They've had mixed success. Despite the fact that numerous studies have found no evidence to support the notion that vaccines cause autism and other chronic illnesses, a growing number of parents are refusing to vaccinate their children.
Researchers now link falling immunization rates to recent resurgences of vaccine-preventable diseases. In 2010, California saw 9,120 cases of whooping cough, more than any year since the whooping cough vaccine was introduced in the 1940s. Ten infants too young to be vaccinated died of whooping cough during the outbreak. The CDC warns that events like these will become more frequent and harder to control if vaccination rates continue to fall.
Fears over the safety of vaccines are understandable. The CDC vaccination schedule calls for children to receive up to 14 inoculations by the age of six – many of them vaccines developed within the last twenty years. Many parents distrust these vaccines; worried about the potential for risks and long-term side effects. Research, however, shows that most of our biggest fears about vaccinations are unfounded. These eight major vaccine myths that research has shown to be baseless:
Myth #1: Vaccines cause autism.The widespread fear that vaccines increase risk of autism originated with a 1997 study published by Andrew Wakefield, a British surgeon. The article was published in The Lancet, a prestigious medical journal, suggesting that the measles, mumps, rubella (MMR) vaccine was increasing autism in British children.
The paper has since been completely discredited due to serious procedural errors, undisclosed financial conflicts of interest, and ethical violations. Andrew Wakefield lost his medical license and the paper was retracted from The Lancet.
Nonetheless, the hypothesis was taken seriously, and several other major studies were conducted. None of them found a link between any vaccine and the likelihood of developing autism.
Today, the true causes of autism remain a mystery, but to the discredit of the autism-vaccination link theory, several studies have now identified symptoms of autism in children well before they receive the MMR vaccine. And even more recent research provides evidence that autism develops in utero, well before a baby is born or receives vaccinations.
In some cases, natural immunity — meaning actually catching a disease and getting sick– results in a stronger immunity to the disease than a vaccination. However, the dangers of this approach far outweigh the relative benefits. If you wanted to gain immunity to measles, for example, by contracting the disease, you would face a 1 in 500 chance of death from your symptoms. In contrast, the number of people who have had severe allergic reactions from an MMR vaccine, is less than one-in-one million.
Myth #4: Vaccines contain unsafe toxins.People have concerns over the use of formaldehyde, mercury or aluminum in vaccines. It's true that these chemicals are toxic to the human body in certain levels, but only trace amounts of these chemicals are used in FDA approved vaccines. In fact, according to the FDA and the CDC, formaldehyde is produced at higher rates by our own metabolic systems and there is no scientific evidence that the low levels of this chemical, mercury or aluminum in vaccines can be harmful. See section III of this guide to review safety information about these chemicals and how they are used in vaccines.
Myth #5: Better hygiene and sanitation are actually responsible for decreased infections, not vaccines.Vaccines don't deserve all the credit for reducing or eliminating rates of infectious disease. Better sanitation, nutrition, and the development of antibiotics helped a lot too. But when these factors are isolated and rates of infectious disease are scrutinized, the role of vaccines cannot be denied.
One example is measles in the United States. When the first measles vaccine was introduced in 1963, rates of infection had been holding steady at around 400,000 cases a year. And while hygienic habits and sanitation didn't change much over the following decade, the rate of measles infections dropped precipitously following the introduction of the vaccine, with only around 25,000 cases by 1970. Another example is Hib disease. According to CDC data, the incidence rate for this malady plummeted from 20,000 in 1990 to around 1,500 in 1993, following the introduction of the vaccine.
Myth #6: Vaccines aren't worth the risk.Despite parent concerns, children have been successfully vaccinated for decades. In fact, there has never been a single credible study linking vaccines to long term health conditions.
As for immediate danger from vaccines, in the form of allergic reactions or severe side effects, the incidence of death are so rare they can't even truly be calculated. For example, only one death was reported to the CDC between 1990 and 1992 that was attributable to a vaccine. The overall incidence rate of severe allergic reaction to vaccines is usually placed around one case for every one or two million injections.
Myth #7: Vaccines can infect my child with the disease it's trying to prevent.Vaccines can cause mild symptoms resembling those of the disease they are protecting against. A common misconception is that these symptoms signal infection. In fact, in the small percentage (less than 1 in one million cases) where symptoms do occur, the vaccine recipients are experiencing a body's immune response to the vaccine, not the disease itself. There is only one recorded instance in which a vaccine was shown to cause disease. This was the Oral Polio Vaccine (OPV) which is no longer used in the U.S. Since then, vaccines have been in safe use for decades and follow strict Food and Drug Administration (FDA) regulations.
Myth #8: We don't need to vaccinate because infection rates are already so low in the United States.Thanks to "herd immunity," so long as a large majority of people are immunized in any population, even the unimmunized minority will be protected. With so many people resistant, an infectious disease will never get a chance to establish itself and spread. This is important because there will always be a portion of the population – infants, pregnant women, elderly, and those with weakened immune systems – that can't receive vaccines.
But if too many people don't vaccinate themselves or their children, they contribute to a collective danger, opening up opportunities for viruses and bacteria to establish themselves and spread.
Not to mention, as the Centers for Disease Control (CDC) warn, international travel is growing quickly, so even if a disease is not a threat in your country, it may be common elsewhere. If someone were to carry in a disease from abroad, an unvaccinated individual will be at far greater risk of getting sick if he or she is exposed.
Vaccines are one of the great pillars of modern medicine. Life used to be especially brutal for children before vaccines, with huge portions being felled by diseases like measles, smallpox, whooping cough, or rubella, to name just a few. Today these ailments can be completely prevented with a simple injection.
So as science continues to advance and tackle new challenges, people should not forget how many deaths and illnesses vaccines have prevented, and how they continue to protect us from potentially devastating forms of infectious disease.
Nine COVID-19 Myths That Just Won’t Go Away
As the world continues to battle the coronavirus, it is also fighting a different sort of epidemic: misinformation. This “infodemic” is just as harmful as COVID-19 itself, leading people to downplay the severity of the disease and ignore public health advice in favor of unproved treatments or “cures.” A recent survey by the John S. and James L. Knight Foundation and Gallup found that four in five Americans say the online spread of misinformation is the biggest problem facing the media. Even with widely available evidence to the contrary, beliefs are hard to change. Here are some of the most insidious falsehoods about the pandemic, and why they are wrong.
Myth 1: The novel coronavirus was engineered in a lab in China.
Because the pathogen first emerged and began infecting people in Wuhan, China, President Donald Trump has claimed—without evidence—that it started in a laboratory there. Some conspiracy theorists have even speculated it was engineered as a bioweapon, although U.S. intelligence agencies have categorically denied this possibility, stating that the intelligence community “concurs with the wide scientific consensus that the COVID-19 virus was not manmade or genetically modified.” No credible evidence has emerged to support an accidental lab release either. As Scientific American reported earlier this year, Chinese virologist Shi Zhengli—who studies bat coronaviruses and whose laboratory Trump and others had suggested was COVID-19’s source—compared the pathogen’s sequence against that of other coronaviruses her team had sampled from bat caves and found that it did not match any of them. Zhengli also explained in detail why her lab could not have been the source of the virus in a lengthy response in Science. In reaction to calls for an independent, international investigation into how the virus originated, China has invited researchers from the World Health Organization to discuss the scope of such a mission. But the evidence suggests SARS-CoV-2 was not created in a lab.
Myth 2: Wealthy elites intentionally spread the virus to win power and profit.
In a video from a conspiracy theory film entitled Plandemic and a book she co-authored, a woman named Judy Mikovits, who once published a high-profile, now retracted study on chronic fatigue syndrome, makes unsubstantiated claims about National Institute of Allergy and Infectious Diseases director Anthony Fauci and Microsoft co-founder Bill Gates, suggesting they have used their power to profit from disease. Science and the Web site PolitiFact have fact-checked some of the film’s claims, many of which appear elsewhere in this article. The video was widely shared by anti-vaxxers and the conspiracy theory group QAnon. It garnered more than eight million views on YouTube, Facebook, Twitter and Instagram before it was taken down because of its false statements. Yet the large number of people who watched it suggests misinformation spreads perniciously.
Myth 3: COVID-19 is no worse than the flu.
Starting in the early days of the pandemic, Trump repeatedly claimed that the disease is not more dangerous than seasonal influenza. But on September 9 the Washington Post published recordings of Trump telling journalist and author Bob Woodward—in interviews in early February and late March—that the president knew COVID-19 was more deadly than the flu and that he wanted to play down its severity. Although COVID-19’s exact mortality rate is hard to pin down, epidemiologists suspect it is far higher than that of the flu. The Centers for Disease Control and Prevention estimates that the latter causes roughly 12,000 to 61,000 deaths per year in the U.S. By contrast, COVID-19 has caused more than 191,000 deaths in the country as of this writing.*
Many people also have partial immunity to the flu because of vaccination or prior infection, whereas most of the world has not yet encountered COVID-19. So no, coronavirus is not “just the flu.”
Myth 4: You don’t need to wear a mask.
Although early guidance on masks from the CDC and the WHO was confusing and inconsistent, there is now a strong consensus among public health authorities—supported by numerous studies—that wearing a face covering can limit the transmission of the coronavirus through small exhaled droplets. Masks have long been known as an effective means of source control (preventing a sick patient from spreading a disease to others), but the early guidance was based, in part, on the fact that there was a shortage of high-quality “N95” and surgical masks. We now know that cloth face masks can be an effective alternative. But despite the evidence, many people still refuse to wear one, considering it a violation of civil liberties or emasculating. Georgia’s governor Brian Kemp went so far as to sign an executive order banning city governments from implementing mask mandates. And he sued Atlanta’s mayor Keisha Lance Bottoms when she instituted one, although he has now dropped the lawsuit. But as coronavirus cases have spiked around the U.S. in recent months, even states that were once staunch holdouts have now implemented mask orders.
Myth 5: Hydroxychloroquine is an effective treatment.
When a small, now widely criticized study in France suggested the malaria drug hydroxychloroquine might be effective at treating the disease, Trump and others seized on it and have continued to tout the medication despite growing evidence that it does not benefit COVID-19 patients. In a tweet, Trump called the hydroxychloroquine treatment “one of the biggest game changers in the history of medicine,” and he has mentioned it repeatedly in his public coronavirus briefings. The Food and Drug Administration initially issued an emergency use authorization for the drug, but the agency later warned against its use because of the risk of heart problems and ultimately revoked its authorization. Several studies have shown that hydroxychloroquine does not protect against COVID-19 in those who are exposed. And in June the National Institutes of Health halted its clinical trial of the medication, stating that while it was not harmful to patients, it did not provide any benefit. Yet Trump continues to hype the drug. Just a few weeks ago, he retweeted a video—viewed tens of millions of times before social media companies took it down—featuring Stella Immanuel, a Houston, Tex.–based physician (who has made questionable assertions in the past, including that doctors had used alien DNA in treatments and that demons cause certain medical conditions by having sex with people in their dreams) claiming hydroxychloroquine is an effective treatment for COVID-19.
Myth 6: The Black Lives Matter protests led to increased transmission.
When thousands of people started taking to the streets in late May and June to protest the police killing of George Floyd and violence against Black Americans, some people questioned whether the mass gatherings would cause a spike in coronavirus cases. But despite the concerns of Republicans such as Representative Jim Jordan of Ohio that the demonstrations pose as big a risk as going to church or the gym, such a marked increase from the protests has not been observed. A white paper analysis of protests in 315 of the largest U.S. cities by the National Bureau of Economic Research found no evidence that they led to more COVID-19 cases or deaths. And those who did not attend the protests may actually have stayed home more than they would have otherwise. The fact that the demonstrations happened outdoors, where the risk of transmission is much lower, and that many protesters wore masks likely prevented superspreading events. Meanwhile, as states have reopened, there has been a notable increase in cases tied to bars and restaurants, as well as other indoor environments—likely because of the risk of airborne spread.
Myth 7: Spikes in cases are because of increased testing.
As coronavirus cases began surging in many parts of the U.S. in recent months, Trump has frequently claimed that these spikes are merely to the result of more people being tested. He has tweeted that “without testing ... we would be showing almost no cases” and has said in interviews that the reason they appear to have gone up is because of increased testing. If that scenario were true, we would expect the percentage of positive tests to go down. But numerous analyses have shown the opposite. The rate has risen in many states with big outbreaks (such as Arizona, Texas and Florida), while it has decreased in those that have controlled their outbreaks (such as New York), indicating that the national increase in positive tests reflects a true increase in cases.
Myth 8: We can achieve herd immunity by letting the virus spread through the population.
Early on in the pandemic, some speculated that the polices chosen by the U.K. and Sweden gave the impression that they planned on letting the virus circulate through their population until they reached herd immunity—the point at which enough people are immune to the virus to prevent it from spreading to others. (Both nations’ governments have denied that this idea was their official strategy, but the U.K. was late to issue a full lockdown, and Sweden had decided against widespread restrictions.) There is a fundamental flaw with this approach, however: Experts estimate that roughly 60 to 70 percent of people would need to get COVID-19 to achieve herd immunity. And given the relatively high mortality rate of the disease, letting it infect that many individuals could lead to millions of deaths. That tragedy is what happened during the 1918 influenza pandemic, in which roughly 50 million people are thought to have perished. The U.K.’s COVID-19 death rate is among the world’s highest. Sweden, for its part, has had significantly more deaths than neighboring countries, and its economy has suffered, despite not shutting down. It is likely that many lives could have been saved if these countries had acted sooner.
Myth 9: Any vaccine will be unsafe and a bigger risk than getting COVID-19.
As scientists race to develop a vaccine against the disease, worrying reports have emerged that many people may refuse to get one once it is available. Conspiracy theories about potential vaccines have circulated among anti-vax groups and in viral videos. In Plandemic, Mikovits falsely claims that any COVID-19 vaccine will “kill millions” and that other vaccines have done so (in fact, vaccines save millions of lives each year). Another conspiracy theory asserts that Bill Gates has a secret plan to use vaccines to implant trackable microchips in people; Gates has denied the claim, which is not supported by evidence. Most Americans still support vaccination, yet the few voices of opposition have been growing. A recent study observed that although clusters of anti-vaxxers on Facebook are smaller than pro-vaccination groups, they are more heavily interconnected with clusters of undecided people. A recent Gallup poll found that one in three Americans would not get a COVID-19 vaccine if it were available today, with Republicans being less likely to be vaccinated than Democrats. There is good reason to be cautious about the safety of a new vaccine, but that need for prudence is why the top contenders are currently conducting large-scale clinical trials in tens of thousands of people to determine safety and efficacy. If one or more of them pass muster, it will be critical for people to get vaccinated to save lives—including, perhaps, their own.
Nine COVID-19 Myths That Just Won't Go Away - Scientific American
https://www.scientificamerican.com/article/nine-covid-19-myths-that-just-wont-go-away/
10 Common Vaccine Myths Busted
Vaccines are widely considered one of the greatest inventions of mankind.
The World Health Organization (WHO) estimates that vaccines prevented over 10 million deaths between 2010 and 2015, and many millions more were protected from illness.
Despite this, there are growing anti-vaccination and vaccine hesitancy movements in Western countries.
Among other problems, these movements caused significant measles outbreaks in the United States, where the potentially deadly virus was once considered eliminated.
There is a lot of misinformation and misconceptions about vaccines that contribute to this growing problem. Here are the facts behind some of the most common vaccine myths.
Myth 1: You can delay routine vaccinations until the coronavirus pandemic is over.
Adult vaccines and childhood vaccines are essential for maintaining health and wellness.
Both the American Academy of Pediatrics and the Centers for Disease Control and Prevention recommend staying up-to-date on routine vaccinations during the pandemic.
Delaying vaccination can be harmful to your health and the health of your community.
In-person care is available across the state at University of Maryland Medical System hospitals and practices during the pandemic. Find out what we're doing to keep patients safe.
Myth 2: Vaccines can make you sick.
Vaccines will not make you sick.
Some people can experience mild side effects from some vaccines, such as soreness at the injection site or a low-grade fever, but they dissipate quickly. According to WHO, serious side effects from vaccines rarely occur. In fact, many adverse effects are so rare that their risk cannot be accurately assessed statistically.
Myth 3: Vaccines contain toxic ingredients.
Dosage is everything when it comes to toxicity.
Any substance—even water—can be toxic in large doses. Some vaccines contain ingredients like formaldehyde and aluminum, but these trace amounts are so small that they're not considered toxic or harmful.
The gelatin and egg proteins featured in some flu vaccines can cause allergic reactions in very rare cases. Those affected typically have a history of severe allergies to gelatin or eggs. If you have an allergy to any of the ingredients in the vaccine, talk to your doctor or the person administering your vaccine.
Myth 4: Vaccines can overload your immune system.
Children often require a lot of vaccinations within a short period of time. Luckily, there is no need to worry.
The immune system is resilient and isn't negatively affected by receiving simultaneous vaccines. There's also no evidence that spacing out vaccines is safer for children. In fact, delaying childhood vaccinations can cause community outbreaks of preventable diseases like measles or chickenpox. A 2015 study showed that only 1% of pediatricians thought vaccines should be spread out.
Myth 5: Natural immunity is healthier and more effective than vaccine-induced immunity.
Vaccines allow you to build immunity without the damaging effects that vaccine-preventable diseases can have.
These diseases can cause serious health problems and even be life-threatening. For example, Haemophilus influenzae type b (Hib) can cause intellectual disability and measles can lead to death. All of these effects can be avoided by simply getting vaccinated.
When administered properly and in the recommended quantities, all vaccines provide you with the protection that you need. In some cases, a single natural infection can invoke a greater immune response than a single vaccine, which is why some vaccines require multiple doses. However, this makes no difference when it comes to preventing infection.
Myth 6: If everyone around me is immune, then I don't need to be vaccinated.
Getting vaccinated is like wearing a mask – it isn't just about protecting you, but also your community.
Most vaccine-preventable diseases spread through person-to-person contact. When one person in a community gets the disease, it can easily spread to other people. The more people who are vaccinated, the fewer chances a disease has to spread.
Myth 7: We don't get vaccine-preventable diseases in the United States.
Diseases that were once common in the United States, like measles or polio, are now rare or even eliminated completely because generations of people were vaccinated to protect themselves and their communities.
In our globalized world, the potential exposure to vaccine-preventable diseases is only a plane ride away. As the coronavirus pandemic has painfully reminded us, if one country has an outbreak, it's the world's concern. In all of human history, smallpox is the only disease to be eradicated from the plant completely.
Failing to get vaccinated can put yourself and your entire community at risk.
Myth 8: The flu vaccine protects you against COVID-19.
There is no evidence to support the claim that the flu vaccine protects against coronavirus.
However, it's still important to get both of these vaccines. In fact, getting your flu vaccine is even more important in 2020. If you fail to get your flu vaccine, you could potentially be infected with coronavirus and the flu at the same time, putting strain on both your health and our health care system.
Myth 9: Vaccines can cause autism.
Vaccines don't cause autism.
This claim stems from a discredited and retracted study that linked the measles, mumps and rubella (MMR) vaccine to autism. Unfortunately, this flawed study has kicked off a resilient storm of misinformation.
Hundreds of studies across the globe have shown time and time again that there is no connection, but a 2016 national study revealed 16.5% of parents or primary caregivers of autistic children believed vaccines caused their child's autism.
Myth 10: Vaccines are used to microchip people.
The internet can be beneficial for learning more about your health, but it can also be fertile ground for misinformation -- particularly during the coronavirus pandemic.
There are some claims that vaccines are or will be used to microchip people so they can be tracked or controlled through 5G cell phone towers. This is not only false, but impossible. Evidence suggests that this conspiracy theory was spread by people seeking to sow disinformation and confusion among Americans.
There are ways to find reliable health information online, but the best thing to do if you have questions about your health is to speak to a doctor.
10 Common Vaccine Myths Busted | University of Maryland Medical System
https://www.umms.org/coronavirus/covid-vaccine/facts/myths-busted
Common COVID-19 Vaccine Myths Explained
No, the vaccine will not alter your DNA or give you COVID-19
Even if you understand the scientific process, trust medical experts and know how important vaccines are for fighting infectious diseases, you might still have some questions or concerns about the new COVID-19 vaccines – especially with so many rumors floating around online.
It’s normal and healthy to have questions, says Thaddeus Stappenbeck, MD, PhD, Chairman of the Department of Inflammation and Immunity at Cleveland Clinic’s Lerner Research Institute.
“These are new therapeutics and it’s totally reasonable to be asking constructive questions with an open mind,” he reassures.
That said, it’s also important to seek out trusted sources of information. Here, Dr. Stappenbeck helps set the record straight on some common questions, concerns and myths that have emerged about COVID-19 vaccines.
Myth 1: We can’t trust COVID-19 vaccines because they were rushed.
The first vaccines for COVID-19 do involve new technology, and they were developed in record time. But it’s not because there were shortcuts in the process.
The new technology at the center of Pfizer’s and Moderna’s COVID-19 vaccines is called messenger RNA, or mRNA. While this is the first time it’s being widely used in a vaccine for the public, researchers have actually been working on this vaccine strategy for more than three decades.
“It was a lucky thing that the technology has been robustly developed quite well over the last few years and tested in several animal models of infection, so we knew that it was safe and worked quite well in these animal models,” Dr. Stappenbeck says.
“When COVID-19 came around, this was an obvious opportunity to use this novel technology, and vaccine developers were poised to do it.”
The companies put their vaccines through rigorous clinical trials involving tens of thousands of volunteers. In the U.S., the Food and Drug Administration requires them to follow up with volunteers for up to two years after receiving the vaccines to make sure they are safe and effective. Because of how prevalent COVID-19 is, it only took a few months for the clinical trials to collect enough data to make an initial evaluation. The FDA, as well as an independent panel of vaccine experts, closely scrutinized the data from those trials and deemed Pfizer’s and Moderna’s vaccines safe and effective for emergency use. Similar independent panels in several other countries are in agreement.
Myth 2: The vaccine will give me COVID-19.
Vaccines prime your immune system to recognize and fight off a disease, but they don’t actually cause an infection.
The first two COVID-19 vaccines that are available in the U.S. contain a strand of genetic material called mRNA. When the mRNA enters your cells, it instructs them to make a piece of the “spike” protein that’s present on the coronavirus that causes COVID-19. Those protein pieces don’t actually harm your body, but they do trigger your immune system to mount a response to fight them off.
You might have some fatigue, muscle aches, a headache or a fever after you get the vaccine. That’s normal with any vaccine – it’s a sign that your immune system is responding.
Myth 3: We don’t know what’s in these vaccines.
Both Pfizer and Moderna have published the ingredient lists for their vaccines. In addition to the star ingredient, the COVID-19 mRNA for the spike protein, both vaccines contain lipids (fats) that help deliver the mRNA into your cells and a few other common ingredients that help maintain the pH and stability of the vaccine. Despite theories circulated on social media, they do not contain microchips or any form of tracking device.
Myth 4: These vaccines will alter my DNA.
The vaccines use mRNA to instruct our cells to make a piece of the coronavirus’s hallmark spike protein in order to spark an immune system response. Once the mRNA does that, our cells break it down and get rid of it.
“Messenger RNA is something that’s made from DNA, but it’s not designed to integrate with our DNA, and it doesn’t permanently change our genome and who we are in any way,” Dr. Stappenbeck says.
Myth 5: I already had COVID-19, so I won’t benefit from the vaccine.
We don’t yet know how long natural immunity to COVID-19 lasts, Dr. Stappenbeck says. Right now, it seems that getting COVID-19 more than once is not common, but there are still many questions that remain unanswered. Experts say that, even if you’ve had COVID-19, it would still be appropriate for you to get the vaccine to make sure you’re protected.
Myth 6: Since COVID-19’s survival rate is so high, I don’t need a vaccine.
It’s true that most people who get COVID-19 are able to recover. But it’s also true that some people develop severe complications. So far, more than 1.7 million people around the world have died from COVID-19 – and that doesn’t account for people who survived but needed to be hospitalized. Because the disease can damage the lungs, heart and brain, it may also cause long-term health problems that experts are still working to understand.
There’s another reason to consider getting the vaccine: It protects those around you. Even if COVID-19 doesn’t make you very sick, you could pass it on to someone else who might be more severely affected. Widespread vaccination protects populations, including those who are most at risk and those who can’t be vaccinated. It will be important for ending the pandemic.
Myth 7: Once I get the vaccine, I won’t have to wear a mask or worry about social distancing.
Even if you get the vaccine, you should continue to wear a mask around others, wash your hands and practice physical distancing. There are a few reasons for this. The first is that both of the authorized vaccines require two doses given three to four weeks apart to achieve the best possible immunity.
When you get your first shot, you don’t become immediately immune. “It takes at least a week to 10 days for your body to begin to develop antibodies, and then those antibodies continue to increase over the next several weeks,” Dr. Stappenbeck says.
The second is that these vaccines were developed and tested for their ability to prevent severe illness and death from COVID-19. It’s not clear whether they also protect against asymptomatic infection and spread.
“There will be ongoing studies to evaluate this question, but it will be some time before we actually know,” Dr. Stappenbeck says. “So after you get the vaccine, you should still take steps to protect other people who haven’t been vaccinated yet.”
Myth 8: Now that we have vaccines, the pandemic will be over very soon.
“I would love to say that we’re going to flip a switch and everything’s going to be back to normal, but it’s actually going to take a long time for us to be able to vaccinate an adequate number of people to where we’ll start to see the cases really dropping,” Dr. Stappenbeck explains.
In order to achieve what’s called herd immunity – the point at which the disease is no longer likely to spread – about 70% of the population will need to have been vaccinated or infected, he says. But the companies that make these vaccines can only make so many at a time. So the vaccines will be distributed in phases, with priority given to people with greatest need. They may not be widely available to the general public until several months into 2021.
For now, we should all continue to do our part to help slow the spread of the virus, including wearing a mask, washing our hands and physical distancing.
If you have more questions about the vaccine, talk with your trusted healthcare provider or look to reliable sources like the Centers for Disease Control and Prevention or the World Health Organization.
Myth 9: The vaccine will cause infertility.
Because the COVID-19 vaccines do not contain the live virus (remember, it’s an mRNA vaccine), they are not thought to cause increased risk of infertility, first or second trimester loss, still birth or congenital anomalies. Additionally, there is no evidence to suggest that the vaccine is a risk to a breastfeeding baby.
Common COVID-19 Vaccine Myths Explained – Cleveland Clinic
https://health.clevelandclinic.org/common-covid-19-vaccine-myths-explained/
History of Anti-vaccination Movements | History of Vaccines
Health and medical scholars have described vaccination as one of the top ten achievements of public health in the 20th century.[1] Yet, opposition to vaccination has existed as long as vaccination itself[2] (indeed, the pre-vaccination practice of variolation came under criticism as well: see our timeline for details). Critics of vaccination have taken a variety of positions, including opposition to the smallpox vaccine in England and the United States in the mid to late 1800s, and the resulting anti-vaccination leagues; as well as more recent vaccination controversies such as those surrounding the safety and efficacy of the diphtheria, tetanus, and pertussis (DTP) immunization, the measles, mumps, and rubella (MMR) vaccine, and the use of a mercury-containing preservative called thimerosal.
Smallpox and the Anti-vaccination Leagues in England
Widespread smallpox vaccination began in the early 1800s, following Edward Jenner’s cowpox experiments, in which he showed that he could protect a child from smallpox if he infected him or her with lymph from a cowpox blister. Jenner’s ideas were novel for his time, however, and they were met with immediate public criticism. The rationale for this criticism varied, and included sanitary, religious, scientific, and political objections.
For some parents, the smallpox vaccination itself induced fear and protest. It included scoring the flesh on a child’s arm, and inserting lymph from the blister of a person who had been vaccinated about a week earlier. Some objectors, including the local clergy, believed that the vaccine was “unchristian” because it came from an animal.[3] For other anti-vaccinators, their discontent with the smallpox vaccine reflected their general distrust in medicine and in Jenner’s ideas about disease spread. Suspicious of the vaccine’s efficacy, some skeptics alleged that smallpox resulted from decaying matter in the atmosphere.[4] Lastly, many people objected to vaccination because they believed it violated their personal liberty, a tension that worsened as the government developed mandatory vaccine policies.[3]
The Vaccination Act of 1853 ordered mandatory vaccination for infants up to 3 months old, and the Act of 1867 extended this age requirement to 14 years, adding penalties for vaccine refusal. The laws were met with immediate resistance from citizens who demanded the right to control their bodies and those of their children.[3] The Anti Vaccination League and the Anti-Compulsory Vaccination League formed in response to the mandatory laws, and numerous anti-vaccination journals sprang up.[2]
The town of Leicester was a particular hotbed of anti vaccine activity and the site of many anti-vaccine rallies. The local paper described the details of a rally: “An escort was formed, preceded by a banner, to escort a young mother and two men, all of whom had resolved to give themselves up to the police and undergo imprisonment in preference to having their children vaccinated…The three were attended by a numerous crowd…three hearty cheers were given for them, which were renewed with increased vigor as they entered the doors of the police cells.”[5] The Leicester Demonstration March of 1885 was one of the most notorious anti-vaccination demonstrations. There, 80,000-100,000 anti-vaccinators led an elaborate march, complete with banners, a child’s coffin, and an effigy of Jenner.[3]
Such demonstrations and general vaccine opposition lead to the development of a commission designed to study vaccination. In 1896 the commission ruled that vaccination protected against smallpox, but suggested removing penalties for failure to vaccinate. The Vaccination Act of 1898 removed penalties and included a “conscientious objector” clause, so that parents who did not believe in vaccination’s safety or efficacy could obtain an exemption certificate.[2]
Smallpox and the Anti-vaccination Leagues in the United States
Toward the end of the 19th century, smallpox outbreaks in the United States led to vaccine campaigns and related anti-vaccine activity. The Anti Vaccination Society of America was founded in 1879, following a visit to America by leading British anti-vaccinationist William Tebb. Two other leagues, the New England Anti Compulsory Vaccination League (1882) and the Anti-vaccination League of New York City (1885) followed. The American anti-vaccinationists waged court battles to repeal vaccination laws in several states including California, Illinois, and Wisconsin.[2]
In 1902, following a smallpox outbreak, the board of health of the city of Cambridge, Massachusetts, mandated all city residents to be vaccinated against smallpox. City resident Henning Jacobson refused vaccination on the grounds that the law violated his right to care for his own body how he knew best. In turn, the city filed criminal charges against him. After losing his court battle locally, Jacobson appealed to the U.S. Supreme Court. In 1905 the Court found in the state’s favor, ruling that the state could enact compulsory laws to protect the public in the event of a communicable disease. This was the first U.S. Supreme Court case concerning the power of states in public health law. [6],[7]
The Diphtheria, Tetanus, and Pertussis (DTP) Vaccine Controversy
Anti-vaccination positions and vaccination controversies are not limited to the past. In the mid 1970s, an international controversy over the safety of the DTP immunization erupted in Europe, Asia, Australia, and North America. In the United Kingdom (UK), opposition resulted in response to a report from the Great Ormond Street Hospital for Sick Children in London, alleging that 36 children suffered neurological conditions following DTP immunization.[8] Television documentaries and newspaper reports drew public attention to the controversy. An advocacy group, The Association of Parents of Vaccine Damaged Children (APVDC), also piqued public interest in the potential risks and consequences of DTP.
In response to decreased vaccination rates and three major epidemics of whooping cough (pertussis), the Joint Commission on Vaccination and Immunization (JCVI), an independent expert advisory committee in the UK, confirmed the safety of the immunization. Nonetheless, public confusion continued, in part because of diverse opinions within the medical profession. For example, surveys of medical providers in the UK in the late 1970s found that they were reluctant to recommend the immunization to all patients.[9] Additionally, an outspoken physician and vaccine opponent, Gordon Stewart, published a series of case reports linking neurological disorders to DTP, sparking additional debate. In response, the JCVI launched the National Childhood Encephalopathy Study (NCES). The study identified every child between 2 and 36 months hospitalized in the UK for neurological illness, and assessed whether or not the immunization was associated with increased risk. NCES results indicated that the risk was very low, and this data lent support to a national pro-immunization campaign.[10] Members of the APVDC continued to argue in court for recognition and compensation, but were denied both due to the lack of evidence linking the DTP immunization with harm.
The U.S. controversy began with media attention on the alleged risks of DTP. A 1982 documentary, DPT: Vaccination Roulette, described alleged adverse reactions to the immunization and minimized the benefits.[11] Similarly, a 1991 book titled A Shot in the Dark outlined potential risks.[12] As in the UK, concerned and angry parents formed victim advocacy groups, but the counter response from medical organizations, like the Academy of Pediatrics and the Centers for Disease Control and Prevention, was stronger in the United States.[9] Although the media storm instigated several lawsuits against vaccine manufacturers, increased vaccine prices, and caused some companies to stop making DTP,[13] the overall controversy affected immunization rates less than in the UK.
The Measles, Mumps, and Rubella (MMR) Vaccine Controversy
Nearly 25 years after the DTP controversy, England was again the site of anti-vaccination activity, this time regarding the MMR vaccine.
In 1998, British doctor Andrew Wakefield recommended further investigation of a possible relationship between bowel disease, autism, and the MMR vaccine.[14] A few years later, Wakefield alleged the vaccine was not properly tested before being put into use.[15] The media seized these stories, igniting public fear and confusion over the safety of the vaccine.[16] The Lancet, the journal that originally published Wakefield’s work, stated in 2004 that it should not have published the paper.[17] The General Medical Council, an independent regulator for doctors in the UK, found that Wakefield had a “fatal conflict of interest.” He had been paid by a law board to find out if there was evidence to support a litigation case by parents who believed that the vaccine had harmed their children. In 2010, the Lancet formally retracted the paper after the British General Medical Council ruled against Wakefield in several areas. Wakefield was struck from the medical register in Great Britain and may no longer practice medicine there. In January 2011, the BMJ published a series of reports by journalist Brian Deer outlining evidence that Wakefield had committed scientific fraud by falsifying data and also that Wakefield hoped to financially profit from his investigations in several ways.[18]
A large number of research studies have been conducted to assess the safety of the MMR vaccine, and none of them has found a link between the vaccine and autism.[19]
“Green Our Vaccines”
Thimerosal, a mercury containing compound used as a preservative in vaccines,[20] has also been the center of a vaccination and autism controversy. Although there is no clear scientific evidence that small amounts of thimerosal in vaccines cause harm, in July 1999, leading U.S. public health and medical organizations and vaccine manufacturers agreed that thimerosal should be reduced or eliminated from vaccines as a precautionary measure.[20] In 2001, The Institute of Medicine’s Immunization Safety Review Committee issued a report concluding that there was not enough evidence to prove or disprove claims that thimerosal in childhood vaccines causes autism, attention deficit hypersensitivity disorder, or speech or language delay.[21] A more recent report by the committee “favors rejection of a causal relationship between thimerosal-containing vaccines and autism.”[22] Even with this finding, some researchers continue to study the possible links between thimerosal and autism.[23] Today, thimerosal is no longer used in most childhood vaccines, though some forms of influenza vaccine available in multi-dose vials may contain the preservative.[24]
Despite scientific evidence, concerns over thimerosal have led to a public “Green Our Vaccines” campaign, a movement to remove “toxins” from vaccines, for fear that these substances lead to autism. Celebrity Jenny McCarthy, her advocacy group Generation Rescue, and the organization Talk about Curing Autism (TACA) have spearheaded these efforts.[25]
In Conclusion
Although the time periods have changed, the emotions and deep-rooted beliefs—whether philosophical, political, or spiritual—that underlie vaccine opposition have remained relatively consistent since Edward Jenner introduced vaccination.
Sources
1. Centers for Disease Control and Prevention (CDC). Ten great public health achievements -- United States, 1900-1999. MMWR. Atlanta, GA: Centers for Disease Control and Prevention (CDC); 1999;48 (12):241-243. Accessed 01/10/2018.
2. Wolfe, R.M., Sharpe, L.K. Anti-vaccinationists past and present. BMJ. 2002d;325:430-432.
3. Durbach, N. They might as well brand us: Working class resistance to compulsory vaccination in Victorian England. The Society for the Social History of Medicine. 2000;13:45-62.
4. Porter, D., Porter, R. The politics of prevention: Anti-vaccination and public health in 19th century England. (2.8 MB). Medical History. 1988;32:231-252. Accessed 01/10/2018.
5. Williamson, S. Anti-vaccination leagues. (288K) Archives of Diseases in Childhood. 1984;59:1195-1196. Accessed 01/10/2018.
6. Gostin, L. Jacobson vs. Massachusetts at 100 years: Police powers and civil liberties in tension. AJPH. 2005;95:576-581. Accessed 01/10/2018.
7. Albert, M., Ostheimer, K.G., Breman, J.G. The last smallpox epidemic in Boston and the vaccination controversy. N Engl J Med. 2001;344. Accessed 01/10/2018.
8. Kulenkampff, M., Schwartzman, J.S., Wilson, J. Neurological complications of pertussis inoculation. (559K) Arch Dis Child. 1974;49:46-49. Accessed 01/10/2018.
9. Baker, J. The pertussis vaccine controversy in Great Britain, 1974-1986. Vaccine. 2003;21:4003-4011.
10. Miller, D.L., Ross, E.M. National childhood encephalopathy study: An interim report. (469K). Br Med J. 1978;2:992–993. Accessed 01/10/2018.
11. WRC-TV, (Washington, D.C.). DPT : Vaccine Roulette. [Film]; 1982.
12. Coulter, H., Fisher, B.L. A Shot in the Dark. New York: Penguin Group; 1991
13. Gangarosa, E.J., Galazka, A.M., Wolfe, C.R., Phillips, L. M., Gangarosa, R. E., Miller, E., Chen, R.T. Impact of anti-vaccine movements on pertussis control: The untold story. The Lancet. 1998;351:356-361.
14. Wakefield, A. Measles, mumps, and rubella vaccine: Through a dark glass, darkly. Adverse drug reactions and toxicological reviews. 2001;19:265-283. Accessed 01/10/2018.
15. Wakefield, A., Murch, S.A., Linnell, J., Casson, D., Malik, M. Ileal-lymphoid-nodular hyperplasia, non specific colitis, and pervasive developmental disorder in children. The Lancet. 1998;351:637-641.
16. Hackett, A.J. Risk, its perception and the media: The MMR controversy. Community Practitioner. 2008;81:22-25
17. BBC News. Lead researcher defends MMR study. BBC News. Sunday, 22 February, 2004. Accessed 01/10/2018.
18. Deer, B. How the case against the MMR vaccine was fixed. BMJ. 2011;342:c5347. Accessed 01/10/2018. Deer B. How the vaccine was meant to make money. BMJ. 2011;342:c5258. Accessed 01/10/2018. Godlee, F., Smith, J., Marcovitch, H. Wakefield's article linking MMR vaccine and autism was fraudulent. BMJ. 2011;342:c7452. Accessed 01/10/2018.
19. Stratton, K., Gable, A., Shetty, P., McCormick, M. Immunization safety review: Measles-mumps-rubella vaccine and autism. Washington, DC: Institute of Medicine, National Academies Press; 2001. Accessed 01/10/2018.
20. Centers for Disease Control and Prevention (CDC). Information about Thimerosal. Accessed 01/10/2018.
21. Institute of Medicine (IOM). Immunization safety review: Thimerosal - containing vaccines and neurodevelopmental disorders. Washington, DC: National Academies Press; 2001. Accessed 01/10/2018.
22. Institute of Medicine (IOM). Immunization safety review: Vaccines and autism. Washington, DC: National Academies Press; 2004. Accessed 01/10/2018.
23. Centers for Disease Control and Prevention (CDC). Vaccine Safety Datalink (VSD) Project Priority Studies. Accessed 01/10/2018.
24. Centers for Disease Control and Prevention (CDC). Frequently Asked Questions about Thimerosal (Ethyl Mercury). Accessed 01/10/2018.
25. Kluger, J. Jenny McCarthy on autism and vaccines. Time Magazine. 2009. Accessed 01/10/2018.
Despite vaccination’s successes against smallpox, opposition to vaccination continued through the 1920s, particularly against compulsory vaccination. In 1926, a group of health officers visited Georgetown, Delaware, to vaccinate the townspeople. A retired Army lieutenant and a city councilman led an armed mob to force them out, successfully preventing the vaccination attempt.
History of Anti-vaccination Movements | History of Vaccines
https://www.historyofvaccines.org/content/articles/history-anti-vaccination-movements
Vaccine Facts and Myths | Texas Children's Hospital
Myth: My child doesn’t need to be vaccinated because the diseases that vaccines prevent have been eliminated in the United States
Fact: There is a small bit of truth to this myth—vaccines have helped to dramatically reduce, but not eliminate, the number of cases of vaccine-preventable diseases in the U.S. However, diseases such as pertussis (whooping cough), influenza, hepatitis and meningitis are still around and can cause serious illness or even death. It’s also important to remember that visitors, both temporary and permanent, come to the U.S. every day from countries where many of these diseases, almost unheard of in this country, are quite common and visitors may bring these infections with them. While polio and German measles (rubella) have been eliminated from the U.S., they still occur in other countries.
There is always a possibility that you can develop a disease if you have not been vaccinated. Protecting yourself and your family by being vaccinated is the best way to ensure protection against vaccine-preventable diseases. Learn more about vaccine-preventable diseases.
Myth: Healthy children do not need to be immunized
Fact: Vaccines are given to prevent infectious diseases in healthy children who were the victims before vaccines were available. Even healthy children can get very sick and be admitted to the hospital or even die from a vaccine-preventable disease. Vaccinations are an important way of helping your child stay healthy.
Myth: I’m increasing my infant’s chance of developing SIDS if I have him or her vaccinated
Fact: This well-known myth resulted in research to find if there is any connection between sudden infant death syndrome (SIDS) and vaccinations. A review of this research from the Institute of Medicine reported that “all controlled studies that have compared immunized versus non-immunized children have found either no association…or a decreased risk of SIDS among immunized children.”
Myth: Since most vaccines are not 100 percent effective, there’s really no need to get them
Fact: It’s true that vaccines are not effective 100 percent of the time, but that doesn’t mean that you should skip any recommended vaccination. Most vaccines protect against disease 85 percent to 99 percent of the time, making vaccination the best way to avoid these diseases. In addition, for some vaccine-preventable diseases, the seriousness of the disease may be less for someone who has received the vaccine. Finally, the more people who get the vaccine, the less likely the disease will be present in the community where it can spread to people who are unable to get the vaccine either because they are too young or have certain medical conditions. This is called "herd immunity".
Myth: The side effects of vaccines are worse than the diseases they are meant to prevent
Fact: In the great majority of cases, the side effects from vaccines are quite minimal (such as injection-site soreness or a slight fever). Yes, several vaccines do have potentially serious side effects, but they are extremely rare and deaths caused by vaccines are almost unheard of. For example, according to the Vaccine Adverse Event Reporting System, between 1990 and 1992, there was only one reported incident of a death that may have been associated with a vaccine. In many ways, vaccines are victims of their own success. Before vaccines, millions of children contracted measles, polio, Haemophilus influenza type B, pertussis and other serious diseases each year. Thousands died or were seriously damaged. Even with advanced medical care in 2009, serious complications and death occur from vaccine-preventable diseases. Vaccination is the best form of protection.
Myth: It’s not safe to get more than one vaccine at a time
Fact: When parents first read the child-and-adolescent vaccine schedule, it’s not unusual for them to be concerned about how many vaccines are given at one time. However, research has shown it is safe for healthy individuals to receive more than one vaccine at a time. Not only is it safe, but it also protects the person as quickly as possible. It is convenient because parents do not have to make as many visits to their health care providers as they would if they were getting vaccinations one at a time.
Myth: Alternative vaccine schedules are a good idea if you are worried about giving too many vaccines at once
Fact: Alternative vaccine schedules are not a good idea. The current vaccination schedule is designed to protect infants against serious diseases as early as possible. Delaying or splitting up vaccinations leaves children, and the general public, unnecessarily vulnerable to serious diseases. The schedules advocated by Dr. Sears are also cumbersome (12 visits over 2 years) and are not supported by science.
Myth: Some of the illnesses that vaccines prevent are not a big deal
Fact: For some children and adults, diseases like chickenpox (Varicella) or rotavirus lead to a mild illness. But that is certainly not the case for everyone. Chickenpox can cause serious complications, including pneumonia and predisposition to being infected by group A Streptococcus (GAS) and Staphylococcus aureus bacteria, both of which can be life-threatening. Pregnant women who get chickenpox may miscarry or the fetus may have abnormalities, such a skin scars or blindness. Each year in the U.S., rotavirus leads to more than 200,000 emergency room visits, 70,000 hospitalizations, and 20 to 60 deaths. Even healthy children can die from influenza. Since vaccine-preventable diseases area constant threat, vaccination is the best protection.
Myth: Vaccines cause the illnesses they’re supposed to prevent
Fact: This myth almost always surfaces during flu season because other respiratory illnesses are common at this time. In regards to the influenza vaccines, neither the inactivated influenza vaccine (the flu shot) nor the live attenuated influenza vaccine (nasal spray) can cause a person to develop influenza.
In regards to the other vaccines on the schedule approved by the Advisory Committee on Immunization Practices of the Centers for Disease Control and Prevention, the American Academy of Pediatrics and the American Academy of Family Physicians, the chance of contracting the disease a vaccine has been proven to protect against is minimal to impossible. For vaccines that contain live weakened viruses, such as the chickenpox or MMR, a patient may develop a very mild illness that would be much less severe if the person did not receive the vaccination and contracted the disease.
Myth: A preservative used in vaccines causes autism
Fact: Preservatives are used in vaccines to prevent contamination with bacteria or fungi. This myth arose because in the past a mercury-containing preservative called thimerosal was used in vaccines. Thimerosal contains ethylmercury, a different form than naturally occurring mercury.
Naturally occurring mercury or methylmercury, can cause health problems in humans when taken at high levels, but has not been shown to cause autism. Several large studies in the U.S., the United Kingdom and Denmark have shown that children who received vaccines that contained the preservative thimerosal were not at a higher risk of developing autism. In Denmark and in California, the number of children diagnosed with autism rose after thimerosal was removed from all vaccines. These studies were large enough to detect even a small risk of autism if it had been present. The Institute of Medicine in 2004 and the National Vaccine Injury Compensation Program in 2010 rejected claims that thimerosal causes autism.
Thimerosal is no longer used as a preservative in any childhood vaccine except the influenza vaccine. The small amount of mercury contained in the influenza vaccine is much lower than the amount a breast-fed infant receives naturally.
Myth: The MMR (Measles, Mumps, Rubella) vaccine causes autism
Fact: This myth arises because the timing of autism diagnosis often coincides with the time of MMR vaccination (age 15-18 months). Affected children, however, often demonstrate signs of autism before this, suggesting another cause. This myth was exaggerated in 1998 after the journal Lancet published the Wakefield study of 11 children (8 with autism) who had intestinal complaints and developed autism within 1 month of receiving the MMR vaccine. 10 of the paper's authors, as well as the hospital attended by the patients, have since disassociated themselves from the study. In February 2010, the Lancet retracted the paper. The Institute of Medicine in 2004 and the National Vaccine Injury Compensation Program in 2009 rejected a "causal relationship" between MMR and autism. Numerous large-scale population studies examining hundreds and thousands of children who were examined over long time periods have proven that MMR does not cause autism.
Myth: The best place to get an injection is always in the buttocks
Fact: Actually, the buttocks are rarely recommended for vaccine injections because the gluteal region has a significant layer of fat, and there’s a chance of damaging the sciatic nerve. Depending upon if the injection is intramuscular, subcutaneous or intradermal, a vaccine injection will be given in either the thigh (usually only for young infants and toddlers) or upper arm.
Myth: Vaccines are not tested enough
Fact: Before any vaccine is licensed and recommended, it must go through a lengthy testing process in thousands of people to ensure it's safety. After licensure, vaccines are continually monitored for any uncommon and rare side effects by examining disease reports from each health department nationwide and vaccine surveillance systems such as Vaccine Adverse Event Reporting System (VAERS) and Vaccine Safety Datalink (VSD).
Vaccine Facts and Myths | Texas Children's Hospital
Common Immunization Myths and Misconceptions
https://www.immunize.org/catg.d/s8035.pdf
How to respond to vocal vaccine deniers in public
The Effects of Anti-Vaccine Conspiracy Theories on Vaccination Intentions
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0089177
Written Definitions and Examples of Each Denial Technique
| TECHNIQUE | DEFINITION | EXAMPLE |
| Ad Hominem | Attacking a person/group instead of addressing their arguments. | “Climate science can’t be trusted because climate scientists are biased.” |
| Ambiguity | Using ambiguous language in order to lead to a misleading conclusion. | “Thermometer readings have uncertainty which means we don’t know whether global warming is happening.” |
| Anchoring | Depending too heavily on an initial piece of information when making subsequent judgments. | “2.2 million people might have died from COVID-19 so keeping it down to only 130,000 deaths is a good job.” |
| Anecdote | Using personal experience or isolated examples instead of sound arguments or compelling evidence. | “The weather is cold today—whatever happened to global warming?” |
| Blowfish | Focusing on an inconsequential aspect of scientific research, blowing it out of proportion in order to distract from or cast doubt on the main conclusions of the research. | “The hockey stick graph is invalid because it contains statistical errors.” |
| Bulk Fake Experts | Citing large numbers of seeming experts to argue that there is no scientific consensus on a topic. | “There is no expert consensus because 31,487 Americans with a science degree signed a petition saying humans aren’t disrupting climate.” |
| Cherry Picking | Carefully selecting data that appear to confirm one position while ignoring other data that contradicts that position. | “Global warming stopped in 1998.” |
| Contradictory | Simultaneously believing in ideas that are mutually contradictory. | “The temperature record is fabricated by scientists… the temperature record shows cooling.” |
| Conspiracy Theory | Proposing that a secret plan exists to implement a nefarious scheme such as hiding a truth. | “The climategate emails prove that climate scientists have engaged in a conspiracy to deceive the public.” |
|
Fake Debate (false balance) |
Presenting science and pseudoscience in an adversarial format to give the false impression of an ongoing scientific debate. | “Climate deniers should get equal coverage with climate scientists, providing a more balanced presentation of views.” |
|
Fake Experts (appeal to false authority) |
Presenting an unqualified person or institution as a source of credible information. | “A retired physicist argues against the climate consensus, claiming the current weather change is just a natural occurrence.” |
| False Analogy | Assuming that because two things are alike in some ways, they are alike in some other respect. | “Climate skeptics are like Galileo who overturned the scientific consensus about geocentrism.” |
| False Choice | Presenting two options as the only possibilities, when other possibilities exist. | “CO2 lags temperature in the ice core record, proving that temperature drives CO2, not the other way around.” |
|
False Equivalence (apples vs. oranges) |
Incorrectly claiming that two things are equivalent, despite the fact that there are notable differences between them. | “Why all the fuss about COVID when thousands die from the flu every year.” |
| Immune to evidence | Re-interpreting any evidence that counters a conspiracy theory as originating from the conspiracy. | “Those investigations finding climate scientists aren’t conspiring were part of the conspiracy.” |
| Impossible Expectations | Demanding unrealistic standards of certainty before acting on the science. | “Scientists can’t even predict the weather next week. How can they predict the climate in 100 years?” |
| Logical Fallacies | Arguments where the conclusion doesn’t logically follow from the premises. Also known as a non sequitur. | “Climate has changed naturally in the past so what’s happening now must be natural.” |
| Lowered Expectations | Lowering the standard by which you grade a performance or assess evidence. | “Two snapshots of Mars show shrinking ice, so Mars is global warming.” |
|
Magnified Minority |
Magnifying the significance of a handful of dissenting scientists to cast doubt on an overwhelming scientific consensus. | “Sure, there’s 97% consensus but Professor Smith disagrees with the consensus position.” |
| Misrepresentation | Misrepresenting a situation or an opponent’s position in such a way as to distort understanding. | “They changed the name from ‘global warming’ to ‘climate change’ because global warming stopped happening.” |
| Moving Goalposts | Demanding higher levels of evidence after receiving requested evidence. | “Sea levels may be rising but they’re not accelerating.” |
| Nefarious intent | Assuming that the motivations behind any presumed conspiracy are nefarious. | “Climate scientists promote the climate hoax because they’re in it for the money.” |
| Overriding suspicion | Having a nihilistic degree of skepticism towards the official account, preventing belief in anything that doesn’t fit into the conspiracy theory. | “Show me one line of evidence for climate change… oh, that evidence is faked!” |
| Oversimplification | Simplifying a situation in such a way as to distort understanding, leading to erroneous conclusions. | “CO2 is plant food so burning fossil fuels will be good for plants.” |
| Persecuted victim | Perceiving and presenting themselves as the victim of organized persecution. | “Climate scientists are trying to take away our freedom.” |
| Quote Mining | Taking a person’s words out-of-context in order to misrepresent their position. | “Mike’s trick… to hide the decline.” |
| Re-interpreting randomness | Believing that nothing occurs by accident, so that random events are re-interpreted as being caused by the conspiracy. | “NASA’s satellite exploded? They must be trying to hide inconvenient data!” |
| Red Herring | Deliberately diverting attention to an irrelevant point to distract from a more important point. | “CO2 is a trace gas so it’s warming effect is minimal.” |
| Single Cause | Assuming a single cause or reason when there might be multiple causes or reasons. | “Climate has changed naturally in the past so what’s happening now must be natural.” |
| Slippery Slope | Suggesting that taking a minor action will inevitably lead to major consequences. | “If we implement even a modest climate policy, it will start us down the slippery slope to socialism and taking away our freedom.” |
| Slothful Induction | Ignoring relevant evidence when coming to a conclusion. | “There is no empirical evidence that humans are causing global warming.” |
| Something must be wrong | Maintaining that “something must be wrong” and the official account is based on deception, even when specific parts of a conspiracy theory become untenable. | “Ok, fine, 97% of climate scientists agree that humans are causing global warming, but that’s just because they’re toeing the party line.” |
| Straw Man | Misrepresenting or exaggerating an opponent’s position to make it easier to attack. | “In the 1970s, climate scientists were predicting an ice age.” |
| Wishful Thinking | Choosing to believe something is true because we really want it to be true, instead of relying on scientific evidence. | “Forget climate model predictions of warming, I think we’re about to experience global |
https://crankyuncle.com/a-history-of-flicc-the-5-techniques-of-science-denial/
The Top COVID-19 Vaccine Myths Spreading Online
https://www.britannica.com/list/the-top-covid-19-vaccine-myths-spreading-online
WRITTEN BY
HealthGuard, a product of NewsGuard, uses journalists to rate and review the credibility of the hundreds of news and information websites people rely on for health information.
Alissa Eckert, MS and Dan Higgins, MAM/CDC
-
MYTH: The mRNA vaccines being developed for COVID-19 will alter
human DNA.
THE FACTS: Several COVID-19 vaccine candidates rely on messenger ribonucleic acid (mRNA), which carries genetic information needed to make proteins, according to the U.S. National Cancer Institute. These vaccines would instruct cells to produce a protein that resembles part of the COVID-19 virus, triggering the body’s immune system to respond and produce antibodies.
MRNA vaccines are a new technology, but it is not possible for those vaccines to alter your DNA. “This cannot change your genetic makeup,” Dr. Dan Culver, a pulmonologist at Cleveland Clinic, told The Associated Pressin September 2020. “The time that this RNA survives in the cells is relatively brief in the span of hours. What you are really doing is sticking a recipe card into the cell making protein for a few hours.”
-
MYTH: COVID-19 vaccines are not being tested against a placebo in
clinical trials.
THE FACTS: The final phase of clinical testing for COVID-19 vaccine candidates are Phase 3 trials, in which the vaccine is given to tens of thousands of patients. Researchers then compare how many patients become infected with COVID-19 compared to a separate group of patients who received a placebo, to determine the vaccine’s efficacy and safety. All 10 vaccine candidates that have begun Phase 3 trials as of Nov. 3, 2020, are being tested against a placebo, according to the World Health Organization.
-
MYTH: The COVID-19 vaccine will use microchip surveillance
technology created by Bill Gates-funded research.
THE FACTS: There is no vaccine — for COVID-19 or otherwise — with a microchip or other surveillance feature. In December 2019, researchers at MIT, who had received funding from the Bill and Melinda Gates Foundation, published a paper about technology that they developed that can keep a vaccination record on a patient’s skin with an ink-like injection that could be read by smartphone. The technology does not have the capacity to track patients’ movements, Kevin McHugh, a Rice University bioengineering professor who worked on the study while at MIT, told FactCheck.org. The Gates Foundation told FactCheck.org that the research is unrelated to COVID-19.
It is true that Gates has said that “digital certificates” could be used as part of a larger vaccination effort, but there is no evidence that he or his foundation has created technology to track recipients of a COVID vaccine. Digital certificates are used to send encrypted information online, and the Gates Foundation told Reuters: “The reference to ‘digital certificates’ relates to efforts to create an open source digital platform with the goal of expanding access to safe, home-based testing.”
Gates himself denied the claims during an interview on CBS News on July 22, 2020. “There’s no connection between any of these vaccines and any tracking type thing at all. I don’t know where that came from,” he said.
-
MYTH: Dr. Anthony Fauci will personally profit from a COVID-19
vaccine.
THE FACTS: There is no evidence that Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases (NIAID), has personal investments in vaccines being developed for COVID-19. Fauci’s agency is working with pharmaceutical company Moderna on a potential vaccine — one of 202 that are currently in development, according to the World Health Organization — but PolitiFact found no record of a business relationship between Fauci and Moderna in an April 2020 search of the U.S. Securities and Exchange Commission’s database.
-
MYTH: A new law in Colorado will force parents into a
government-run re-education program if they refuse to give their
children a COVID-19 vaccine.
THE FACTS: The School Entry Immunization Bill, signed into law by Colorado’s governor in June 2020, does not make any reference to COVID-19 or a COVID-19 vaccine. The law did toughen the state’s process for obtaining a religious or personal belief vaccine exemption, requiring parents requesting such an exemption to either submit a form signed by a health care provider, or complete what the law calls an “online education module” about vaccine science, produced by the Colorado Department of Public Health and Environment.
-
MYTH: The COVID-19 vaccine has been proven to cause infertility
in 97 percent of its recipients.
THE FACTS: This claim appears to have originated with British YouTuber Zed Phoenix, who claimed that an unnamed source at pharmaceutical company GlaxoSmithKline told him that 61 of the 63 women tested with a COVID-19 vaccine became infertile and that a separate, male-specific vaccine “resulted in decreased testicular size, drop of testosterone levels, and marked atrophy of the prostate.”
Phoenix’s statements about the alleged effects of these vaccines appear to have been taken verbatim from an unrelated 1989 study from the National Institute of Immunology in New Delhi, India, according to Reuters. This research examined the use of anti-fertility vaccines on baboons in discussing future treatment options for human cancer patients whose tumors are affected by fertility hormones. None of the COVID-19 vaccine candidates are gender-specific or are in any way related to fertility.
-
MYTH: COVID-19 vaccines will contain aborted human fetal
tissue.
THE FACTS: Existing vaccines for diseases such as chickenpox and rubella are produced using cell lines descended from fetuses aborted decades ago. According to a June 2020 article published in Science magazine, at least five COVID-19 vaccine candidates are using fetal cell lines: one descended from a fetus aborted in 1972 and another from an abortion performed in 1985.
However, no additional fetal cells are required for the production of any of these vaccines, including those being developed for COVID-19, and no actual fetal tissue is present in these vaccines. The National Catholic Bioethics Center, which consults with the Vatican and Catholics on medical ethics issues and opposes abortion, has stated, “The cells in these lines have gone through multiple divisions before they are used in vaccine manufacture. After manufacture, the vaccines are removed from the cell lines and purified. One cannot accurately say that the vaccines contain any of the cells from the original abortion.”
-
MYTH: The COVID-19 vaccine being developed by Oxford University
and AstraZeneca will turn people into monkeys.
THE FACTS: This false claim is based on the fact that Oxford and AstraZeneca’s vaccine relies on a modified chimpanzee adenovirus intended to generate an immune response to the virus that causes COVID-19. According to The Times of London, the claim is being promoted through memes and video clips as part of a disinformation campaign involving officials in Russian state agencies, specifically targeted at countries where Russia wants to sell its own COVID-19 vaccine.
-
MYTH: Government food stamps will be denied to those who refuse
COVID-19 vaccines.
THE FACTS: The pseudoscience and conspiracy-oriented website Natural News first reported that President-elect Joe Biden’s COVID-19 task force had announced such a policy. However, the article relied on outdated and inaccurate information. Dr. Luciana Borio, a member of the task force, helped write a report from the Johns Hopkins Center for Health Security in July 2020 that mentioned government food stamps in a larger discussion about COVID-19 vaccines. However, the report was not part of the task force, and it did not advocate the denial of food stamps to people who decline to take a COVID-19 vaccine. The report’s lead authors said in a statement to FactCheck.org in November 2020 that they “do NOT advocate that such social supports ever be withheld in connection with an individual’s vaccination status.”
-
MYTH: The U.K. Medicines and Healthcare products Regulatory
Agency (MHRA) will use artificial intelligence to monitor the
safety of COVID-19 vaccines because the agency knows that vaccines
are extremely dangerous.
THE FACTS: It is true that MHRA has awarded a contract to the company Genpact to create an artificial intelligence tool to monitor reports of adverse effects to COVID-19 vaccines. However, the agency states that this is not evidence of foreknowledge of dangers posed by vaccines. Moreover, an adverse event report does not prove that the event or reaction was caused by a vaccine.
In a November 2020 statement to NewsGuard, the MHRA said, “We have a range of resources and technology to support the safety monitoring of any COVID-19 vaccination programme. The use of AI will be one element of that. We take every report of a suspected side effect seriously and we combine the review of these individual reports with statistical analysis of clinical records.”
The agency continued: “Based on the available published reports from the Phase One and Two clinical trials, we don’t currently anticipate any specific safety concerns with COVID-19 vaccines. We expect the general safety profile to be similar to other types of vaccines. A COVID-19 vaccine will only be deployed once it has been proven to be safe and effective through robust clinical trials and approved for use.”
-
MYTH: A document on the FDA website shows that two participants
died as a result of “serious adverse events” from an experimental
COVID-19 vaccine.
THE FACTS: There were two deaths among the 21,000 people in the trial who received Pfizer and BioNtech’s COVID-19 vaccine, but the U.S. Food and Drug Administration did not attribute those deaths to the vaccine.
According to a December 2020 FDA document describing the circumstances of the deaths, “one experienced a cardiac arrest 62 days after vaccination #2 and died 3 days later, and the other died from arteriosclerosis 3 days after vaccination #1.” The document also said in the case of the second death, the participant had “baseline obesity and pre-existing atherosclerosis,” or a narrowing of the arteries.
There were also four deaths reported among the 21,000 trial participants who received a placebo. The deaths “represent events that occur in the general population of the age groups where they occurred, at a similar rate,” according to the FDA document.
To determine the safety of the vaccine, the trial recorded what are called “serious adverse events,” defined by the U.S. National Library of Medicine as any medical event that results in death, hospitalization, or interferes substantially with normal life functions. The FDA document said among the serious events reported in the Pfizer/BioNTech trial, it considered only two as possibly related to the vaccine: a shoulder injury and swollen lymph nodes, a common and typically benign condition.
-
MYTH: The virus mutates so fast that a vaccine will never
work.
THE FACTS: While all viruses mutate constantly, the World Health Organization said in December 2020 that, “SARS-CoV-2, the virus which causes COVID-19, tends to change more slowly than others such as HIV or influenza viruses.” The more rapid changes in influenza viruses are one reason why the flu vaccine is updated annually.
Preliminary laboratory studies released in January 2021 on the first two COVID-19 vaccines authorized for use in the U.S. — one made by Pfizer/BioNTech, the other made by Moderna — found that their vaccines are still effective against a mutation first identified in the U.K known as the B.1.1.7 strain. Although the studies did suggest vaccines being less effective against the B.1.351 mutation found in South Africa, there was no evidence that the mutations would negate the vaccines’ benefits entirely.
“You could diminish the vaccine-induced antibody efficacy by a few fold and still be well within the protective range of the vaccine,” Dr. Anthony Fauci, director of the U.S. National Institute of Allergy and Infectious Diseases, said in a White House briefing on Jan. 27, 2021.
-
MYTH: The head of research at Pfizer said the company’s COVID-19
vaccine contains a protein called syncytin-1 that will result in
female sterilization.
THE FACTS: This claim was based on a petition to the European Medicines Agency from a doctor named Michael Yeadon, apparently the aforementioned “head of Pfizer research.” In fact, Yeadon had left the company in 2011, according to a December 2020 article by The Associated Press.
The petition speculated that the vaccine may create an immune response against a protein vital for the formation of the placenta during pregnancy. However, the vaccine does not contain syncytin-1 and there is no evidence connecting the COVID-19 vaccine to infertility.
Moreover, there is no evidence that the spike protein in the virus that causes COVID-19 and that is being targeted by the vaccine will create an immune response against syncytin-1, scientists say. “Any hint of similarity between syncytin-1 and the SARS-CoV-2 spike protein (which is used as part of the vaccine) is extremely remote,” Brent Stockwell, a biological sciences and chemistry professor at Columbia University, told PolitiFact in December 2020. “There are hardly any parts of the two proteins that are even vaguely similar, and they are far more distinct than would be needed for cross-reactivity of immune responses.”
In a December 2020 statement to The Associated Press, Pfizer spokesperson Jerica Pitts said the company’s COVID-19 vaccine had not been found to cause infertility. “It has been incorrectly suggested that COVID-19 vaccines will cause infertility because of a shared amino acid sequence in the spike protein of SARS-CoV-2 and a placental protein,” she said. “The sequence, however, is too short to plausibly give rise to autoimmunity.”
-
MYTH: COVID-19 vaccine injections, shown during press events
being delivered to health care workers, are fabricated, using
syringes with “disappearing needles.”
THE FACTS: These claims were made in Twitter posts and YouTube clips, using real videos from press events where health care workers received COVID-19 vaccines. One tweet that promoted this claim, using BBC footage of a worker receiving a COVID-19 vaccine injection, attracted 394,000 views between Dec. 16 and 17, 2020.
According to the BBC and Vice News, the injections of the COVID-19 vaccine shown in these videos were delivered using retractable syringes, not “disappearing needles,” where the needlepoint automatically retracted into the barrel of the syringe once the dose of medication was delivered. Retractable syringes are typically used to reduce needlepoint injuries, such as a nurse or a lab worker accidentally puncturing their skin with a used needle and potentially exposing themselves to infection.
Retractable syringes have been in use for years before the COVID-19 vaccine was introduced. A patent for a “retractable needle hypodermic syringe” was granted in the U.S. in 1992.
-
MYTH: A nurse in Alabama died hours after receiving the COVID-19
vaccine.
THE FACTS: According to fact-checking website LeadStories.com, this claim first appeared in screenshots of a text message conversation shared on Facebook on Dec. 15, 2020, by a Facebook account using the name Danielle Tyler.
Facebook posts that shared the screenshots claimed that a 42-year-old nurse who received the COVID-19 vaccine was “found dead eight hours later.” The source for this claim, according to the Facebook posts, was “not an internet rumor, my FB friend’s friend’s aunt.”
In a Dec. 16, 2020, statement to LeadStories.com, the Alabama Department of Public Health said it “has reached out to all hospitals in the state which administered the COVID-19 vaccine and confirmed there have been no deaths of vaccine recipients. The posts are untrue. No person who received a COVID-19 vaccine in Alabama has died.”
The emergency use authorization for the first COVID-19 vaccine, developed by Pfizer and BioNTech, requires that serious adverse events following vaccination, including deaths, have to be reported to the Vaccine Adverse Event Reporting System (VAERS), which is co-operated by the U.S. Food and Drug Administration and the U.S. Centers for Disease Control and Prevention.
In an Dec. 16, 2020, email to PolitiFact, CDC spokesperson Kristin Nordlund said, “I can confirm that as of 4 p.m. ET today that VAERS has received no reports of death after COVID-19 vaccines.”
-
MYTH: The COVID-19 vaccines violate the Nuremberg Code, which
bans medical experiments from being performed on humans without
their consent.
THE FACTS: The Nuremberg Code created a set of medical research ethics principles for what it calls “permissible medical experiments.” According to a June 2020 article by FactCheck.org, the code was created in response to Nazis performing medical experiments on concentration camp prisoners without their consent.
Vaccines that have gone through multiple rounds of testing in clinical trials and have then been approved for widespread use by regulators are not in violation of the Nuremberg Code’s principles. For example, the COVID-19 vaccine developed by Pfizer and BioNTech was authorized for emergency use by the UK Medicines and Healthcare Products Regulatory Agency and the U.S. Food and Drug Administration in 2020 only after it went through multiple clinical trials to demonstrate its safety and efficacy, with the final Phase 3 trial involving 43,000 patients.
“The Nuremberg Code is about doing human experiments, not vaccination,” Dr. Jonathan Moreno, professor of bioethics at the University of Pennsylvania, told Agence France-Presse in a May 2020 article. “The Nuremberg Code is perfectly compatible with vaccination.”
-
MYTH: The COVID-19 vaccines will cause “pathogenic priming” or
“disease enhancement,” meaning that vaccinated individuals will be
more likely to develop severe cases of COVID-19 if they are
infected with the COVID-19 virus.
THE FACTS: COVID-19 vaccines went through multiple clinical trials to determine their safety and efficacy before being authorized for emergency use by regulators.
The final phase 3 trials for two COVID-19 vaccines authorized in the U.S. as of January 2021 — one developed by Moderna and another from Pfizer and BioNTech — involved a combined 36,000 people receiving one of the two vaccines.
Contrary to the claim that the vaccines cause more severe cases of COVID-19, out of the 36,000 people who received the vaccines, only one developed a severe case, according to the results of the Moderna and Pfizer/BioNTechvaccines’ clinical trials, which were both published in the New England Journal of Medicine in December 2020. The single instance of severe COVID-19 among vaccine recipients was observed in the Pfizer/BioNTech trial. Both vaccines were found to be approximately 95 percent effective in preventing COVID-19.
In a November 2020 article published on fact-checking website Health Feedback, Walter Orenstein, a professor at the Emory University School of Medicine in Atlanta, stated that “thus far, there are no data supporting vaccination as a cause of vaccine-induced enhanced disease.”
Correction: An earlier version of this report inaccurately stated there were two severe cases of COVID-19 observed among the 36,000 people who received either the Moderna or Pfizer/BioNTech COVID-19 vaccine. Only one severe case of COVID-19 was reported among vaccine recipients in either trial, both of which were published in December 2020, with the single instance coming in the Pfizer/BioNTech trial. NewsGuard apologizes for the error.
-
MYTH: The COVID-19 vaccine can cause people to develop
COVID-19.
THE FACTS: None of the vaccines authorized for widespread use in the U.S. or Europe as of January 2021 contain the live virus that causes COVID-19 virus. “This means that a COVID-19 vaccine cannot make you sick with COVID-19,” the U.S. Centers for Disease Control and Prevention stated on its website.
However, the CDC did note that the available vaccines require two doses, and it will take some time after vaccination for the body to build immunity against the COVID-19 virus. “That means it’s possible a person could be infected with the virus that causes COVID-19 just before or just after vaccination and still get sick,” the CDC stated. “This is because the vaccine has not had enough time to provide protection.”
COVID-19 cases among fully vaccinated individuals are still possible, because none of the available vaccines have been found to be 100 percent effective in preventing symptomatic cases of COVID-19. Additionally, the vaccines might not prevent asymptomatic infection, meaning vaccine recipients might be able to get infected, show no symptoms, and unwittingly spread the virus, according to the Children’s Hospital of Philadelphia.
-
MYTH: The mRNA vaccines for COVID-19 do not fit the CDC and FDA’s
definitions of a vaccine, which state that vaccines have to both
stimulate immunity and disrupt transmission of a virus.
THE FACTS: This claim was promoted by David Martin, a financial analyst and self-help entrepreneur who operates a YouTube channel pushing COVID-19 conspiracy theories.
As of January 2021, research is ongoing to determine whether COVID-19 vaccines prevent transmission of the COVID-19 virus. However, contrary to Martin’s claim, neither U.S. Centers for Disease Control and Prevention and the U.S. Food and Drug Administration stipulate that vaccines must both provide immunity and block transmission of a virus.
“There are many ways to define it, but CDC describes a vaccine as a product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease,” CDC spokesperson Kristen Nordlund told NewsGuard in a January 2021 email. Similarly, a page on the FDA’s website explaining how vaccines work only mentions preventing disease, not transmission, stating, “Vaccination stimulates the body’s immune system to build up defenses against the infectious bacteria or virus (organism) without causing the disease.”
The two mRNA vaccines authorized for emergency use in the U.S. as of January 2021 would fit those definitions, as clinical trials found that both vaccines are approximately 95 percent effective in preventing COVID-19.
-
MYTH: Hank Aaron’s death is linked to the COVID-19 vaccine.
THE FACTS: Baseball Hall of Famer and Major League Baseball’s one-time home run king Hank Aaron received the Moderna COVID-19 vaccine on Jan. 5, 2021, at the Morehouse School of Medicine. He told The Associated Press at the time that he hoped his willingness to be vaccinated would reduce vaccine hesitancy among Black Americans.
The 86-year-old Aaron died on Jan. 22, 2021. Before his cause of death was disclosed, anti-vaccine activists Robert F. Kennedy Jr. and Del Bigtree, both of whom have repeatedly spread false claims about the safety of vaccines, suggested without evidence that Aaron’s death was caused by the COVID-19 vaccine.
Morehouse College of Medicine spokesperson Nicole Linton denied these claims in an email to NewsGuard, stating, “His passing was not related to the vaccine, nor did he experience any side effects from the immunization. He passed away peacefully in his sleep.”
Three days after his death, the Fulton County Medical Examiner’s Office reported that Aaron died of natural causes. Additionally, Fox 5 Atlantareported that officials at the medical examiner’s office do not believe the COVID-19 vaccine had any adverse effect on Aaron’s health and did not contribute to his death.
-
MYTH: A Tennessee nurse named Tiffany Dover died after receiving
the COVID-19 vaccine on live TV.
THE FACTS: Dover, a nurse at Catholic Health Initiatives (CHI) Memorial Hospital in Chattanooga, Tennessee, received her COVID-19 vaccine during a live broadcast on WRCB-TV on Dec. 17, 2020. During a subsequent interview with the station, she fainted, which she later explained was a common occurrence. “I have a history of having an overactive vagal response and with that, if I have pain from anything, hangnail or if I stub my toe, I can just pass out,” she said.
CHI Memorial Hospital released a video on Dec. 21, 2020, showing Dover with other staff members and confirmed that she is alive and well in statements to WRCB, The Associated Press, and Reuters.
The Daily Beast reported in a January 2021 article that multiple relatives of Dover have confirmed on social media that she is alive, in response to online harassment from anti-vaccine activists. Elisa Myzal, a spokesperson for the Chattanooga Police Department, told the Daily Beast, “The police department isn’t involved in this at all because there’s no crime, no death, no nothing.”
-
MYTH: COVID-19 vaccines are not halal or kosher because they
contain pork products.
THE FACTS: Halal food refers to food that adheres to Islamic law on how food is raised, slaughtered, and prepared. Similarly, kosher food refers to foods that meet Jewish dietary standards. Both religions consider pork products to be forbidden.
Pork gelatin is contained in some vaccines licensed in the U.S., including the measles, mumps, and rubella vaccines. Gelatin is used to “protect vaccine viruses from adverse conditions such as freeze-drying or heat, particularly during transport and delivery,” according to the Children’s Hospital of Philadelphia.
However, the four COVID-19 vaccines that have been authorized for widespread emergency use in the U.S. and Europe — those produced by Pfizer, Moderna, AstraZeneca, and Johnson & Johnson — do not contain pork products, according to a February 2021 article in the Brussels Times.
In fact, Islamic and Jewish authorities, including the British Islamic Medical Association, Assembly of Muslim Jurists of America, the Rabbinical Council of America, and the Board of Deputies of British Jews, have encouraged their communities to get COVID-19 vaccines.
-
MYTH: The trials for COVID-19 vaccines were not designed to show
the vaccines’ effectiveness in preventing severe cases of the
disease.
THE FACTS: In October 2020, the Food and Drug Administration announced that industry requests for emergency authorization of COVID-19 vaccines had to include data on “cases of severe COVID-19 disease among study subjects” in all phases of the vaccines’ clinical trials. This contradicts the claim that the vaccines were only designed for mild cases.
Moreover, clinical trial results for each of the three COVID-19 vaccines authorized in the U.S. — made by Pfizer/BioNTech, Moderna, and Johnson & Johnson — as well as the AstraZeneca vaccine, which has been authorized in the U.K. and the European Union, included data showing that the vaccines were effective in preventing severe cases of COVID-19.
The claim that COVID-19 vaccine trials only demonstrated effectiveness against mild, symptomatic cases and not severe ones appears to be based on COVID-19 vaccine trials’ “primary endpoint,” which the U.S. National Cancer Institute defines as “The main result that is measured at the end of a study to see if a given treatment worked.” For the Pfizer/BioNTech and Moderna vaccine trials, the primary endpoint was based on preventing cases where a participant showed mild symptoms of COVID-19, such as fever, cough, and chills, and then tested positive for the disease.
However, as noted, the trials also measured the vaccines’ efficacy on what are called “secondary endpoints,” defined by the FDA as outcomes in clinical trials “selected to demonstrate additional effects after success on the primary endpoint.” These secondary endpoints include severe COVID-19 cases, the definition of which included respiratory failure, admission to an intensive care unit, or death.
At an October 2020 meeting on the FDA’s vaccine advisory committee, health experts on the committee said concerns that the trials’ primary endpoints meant they could only prove that the vaccines were effective against mild COVID-19 were unfounded. “There simply does not exist an example in vaccinology of vaccines that are effective against mild disease that are not more effective in severe disease,” said Dr. Phillip Krause, deputy director of the FDA’s Office of Vaccines Research and Review.
-
MYTH: American boxer Marvin Hagler’s death is linked to the
COVID-19 vaccine.
THE FACTS: This myth relies on an Instagram post made by boxer Thomas Hearns on March 13, 2021, in which Hearns stated that Hagler was “in ICU fighting the after effects of the vaccine.” Hagler died later that day, and vaccine misinformation sites have used Hearns’ statement to tie Hagler’s death to his COVID-19 vaccination.
There is no evidence that Hagler, who was 66 at the time of his death, died from anything related to a COVID-19 vaccine or vaccine side effects. A statement on the boxer’s official website said that he “died on March 13 of natural causes,” and Hagler’s wife Kay wrote in a post on his official Facebook fan page that Hagler had “passed away unexpectedly at his home here in New Hampshire.”
Kay Hagler wrote in another post on Hagler’s Facebook fan page that it “for sure wasn’t the vaccine that caused his death,” noting that “I was the only person close to him until the last minute, and I am the only person that know [sic] how things went … now is not the time to talk nonsense.” Hearns himself later wrote on Instagram that “this is not an anti vaccine campaign … It’s outrageous to have that in mind during the passing of a King, Legend, Father, Husband and so much more.”
The U.S. Centers for Disease Control and Prevention states on its website that COVID-19 vaccines approved for use in the U.S. “are safe and effective. Millions of people in the United States have received COVID-19 vaccines under the most intense safety monitoring in U.S. history.” The CDC also says that to date, its vaccine adverse event reporting system (VAERS) “has not detected patterns in cause of death that would indicate a safety problem with COVID-19 vaccines.”
-
MYTH: Scientists at Memorial Sloan Kettering Cancer Center have
discovered that mRNA inactivates tumor-suppressing proteins,
meaning that mRNA vaccines used to protect against COVID-19 can
cause cancer.
THE FACTS: This false claim was first promoted by NaturalNews.com, a network of health misinformation sites that NewsGuard has found to have repeatedly published false content. The March 2021 NaturalNews.com article was based on a Memorial Sloan Kettering Cancer Center (MSKCC) study published in August 2018 in the journal Nature. Although that study did find that changes in mRNA can inactivate tumor-suppressing proteins, the research was not connected to mRNA vaccines like those used against COVID-19.
“This article circulating is categorically false, misrepresents the findings of our study and draws incorrect conclusions about vaccine risks,” Jeanne D’Agostino, spokesperson for Memorial Sloan Kettering, told Agence France-Presse in March 2021.
In fact, months before the NaturalNews.com story was published, the cancer center had updated its August 2018 press release about the study, to make it clear that the research did not involve mRNA vaccines. The updated text stated, “It’s important to note that mRNAs are a normal component of all cells and the specific ones discussed here are not involved in mRNA-based vaccines, like the one developed against SARS-CoV-2,” the virus that causes COVID-19.
According to a March 2021 article on Memorial Sloan Kettering Cancer Center’s website, “It’s important to know that none of the COVID-19 vaccines interact with or alter your DNA in any way. They cannot cause cancer.”
-
MYTH: COVID-19 vaccines have been proven to increase the risk of
having a miscarriage.
THE FACTS: A spokesperson for the U.S. Centers for Disease Control and Prevention told Agence France-Presse in February 2021, “To date, no evidence has indicated an increase in miscarriages after Covid-19 vaccines, and no concerning patterns of reporting have been observed.” A February 2021 document from the British Fertility Society and the U.K. Association of Reproductive and Clinical Scientists stated that COVID-19 vaccines “will not affect your risk of having a miscarriage.”
Sources claiming that a link exists between miscarriages and COVID-19 vaccines have frequently cited data from CDC’s Vaccine Adverse Event Reporting System (VAERS) and U.K. Medicines & Healthcare Products Regulatory Agency’s (MHRA) Yellow Card program. Both of these systems collect unverified reports of possible vaccine side effects that can be submitted by anyone, and do not prove that the vaccine caused the reported reaction.
A MHRA spokesperson told Reuters in March 2021, “There is no pattern to suggest an elevated risk of miscarriage related to exposure to the COVID-19 vaccines in pregnancy… Sadly, miscarriage is estimated to occur in about 1 in 4 pregnancies (equal to 25 in 100) in the UK (outside of the pandemic) and most occur in the first 12 weeks (first trimester) of pregnancy, so some miscarriages would be expected to occur following vaccination purely by chance.”
-
MYTH: Vaccines are increasing the number of new variants of the
COVID-19 virus and making vaccinated individuals more likely to
infect others with new super-strains.
THE FACTS: None of the COVID-19 vaccines authorized for emergency use in the U.S. and Europe contain a live COVID-19 virus, and thus cannot create a variant or allow vaccinated individuals to infect others.
Martin Hibberd, a professor of emerging infectious disease at the London School of Hygiene & Tropical Medicine, told NewsGuard in a March 2021 email that the approved vaccines “are not complete viruses and so cannot replicate a new variant that can infect others. Some types of vaccine use attenuated whole viruses and these can generate variants that could theoretically pass on to others, but the COVID-19 vaccines are not of that type and so cannot do that.”
Hibberd also explained that variants that show some resistance to vaccine-acquired immunity could be more easily spread, but this does not mean that the vaccine created those variants. So far, there is no evidence of “resistant strains arising directly as a result of vaccines,” according to Hibberd.
Professor Luke O’Neill, an immunologist at Trinity College Dublin, told Euronews in April 2021 that, “Vaccines bring out the human immune system to kill the virus, that stops it replicating and therefore the chance of variants emerging is decreased.”
-
MYTH: PCR tests used to detect the virus that causes COVID-19 can
also be used to secretly deliver the COVID-19 vaccine, according
to research from Johns Hopkins University.
THE FACTS: This myth misrepresents an animal study by Johns Hopkins researchers and published in the journal Science Advances in October 2020. The study tested devices called theragrippers, which are as small as a speck of dust and can deliver medicine to the gastrointestinal tract, with the goal of improving the efficacy of extended-release drugs.
Unlike the polymerase chain reaction, or PCR, tests used to detect the virus that causes COVID-19 — where a swab is inserted in the nose — the theragrippers in the Johns Hopkins study were administered via the rectum.
Johns Hopkins Medicine told NewsGuard in an April 2021 email, “This nanotechnology has shown promise in a laboratory setting. However, it is still in its infancy and has not been approved for use in humans. Theragrippers have been neither tested nor used for vaccine delivery.”
-
MYTH: Life insurance companies won’t pay out benefits to anyone
who dies after receiving a COVID-19 vaccine because the vaccines
are considered experimental.
THE FACTS: Paul Graham, senior vice president of policy development at the American Council of Life Insurers, addressed this claim in a March 2021 statement on the council’s website. “The fact is that life insurers do not consider whether or not a policyholder has received a COVID vaccine when deciding whether to pay a claim,” Graham said. “Life insurance policy contracts are very clear on how policies work, and what cause, if any, might lead to the denial of a benefit. A vaccine for COVID-19 is not one of them. Policyholders should rest assured that nothing has changed in the claims-paying process as a result of COVID-19 vaccinations.”
The Canadian Life and Health Insurance Association and the Association of British Insurers each released similar statements in March 2021 explaining that COVID-19 vaccinations will have no impact on an individual life insurance coverage or benefits.
Contrary to the claim that the COVID-19 vaccines are considered “experimental,” each of the vaccines authorized for emergency use in the U.S. and Europe had to undergo multiple phases of clinical trials to test their safety and efficacy, although some phases overlapped to shorten development time. That data was then reviewed by health regulators before the vaccines were authorized for emergency use.
-
MYTH: MRNA COVID-19 vaccines can cause an increase in rare
neurodegenerative disorders called prion diseases.
THE FACTS: This claim was based on a January 2021 research articlepublished in the journal Microbiology & Infectious Diseases. The article was written by Dr. J. Bart Classen, an immunologist in Maryland who has previously promoted the false claim that vaccines are linked to diabetes, according to a February 2021 PolitiFact article.
According to the U.S. Centers for Disease Control and Prevention, prion diseases are “a family of rare progressive neurodegenerative disorders that affect both humans and animals.” One such disease is bovine spongiform encephalopathy, more widely known as mad cow disease. The disease is named for prions, which the CDC defines as “abnormal, pathogenic agents that are transmissible and are able to induce abnormal folding of specific normal cellular proteins called prion proteins that are found most abundantly in the brain.”
Classen’s article did assert that mRNA vaccines could cause prion diseases, as well as other neurological conditions such as Alzheimer’s disease, but only cited as evidence of the claim a three-sentence summary of an unspecified analysis of the Pfizer/BioNTech COVID-19 vaccine.
Jacob Yount, an associate professor of microbial infection and immunity at Ohio State University, told The Dispatch in April 2021 that Classen’s study “seems to be based on gibberish presented in a seemingly scientific manner.” Yount said, “mRNA vaccines have a longer history of testing in humans that started several years before the COVID vaccines, and these past vaccines were found to be safe and have not resulted in prion disease. Further, the mRNAs themselves are degraded by our cells in a matter of days, so I do not find any reason to think that the mRNAs delivered to cells in our arm muscle would have a direct effect on proteins in the brain.”
-
MYTH: Being in close proximity to someone who has received a
COVID-19 vaccine can cause unvaccinated women to have a
miscarriage or experience menstrual cycle changes.
THE FACTS: According to an April 2021 article by The Associated Press, it is biologically impossible for unvaccinated women to experience reproductive problems just by being around individuals who have received a COVID-19 vaccine.
A spokesperson for the U.S. National Institutes of Health told Reuters in April 2021, “There is no evidence that individuals vaccinated for COVID-19 can transmit the vaccines to others or that vaccination of one person can have negative health effects on others.” Dr. Taraneh Shirazian, an NYU Langone gynecologist, told The Associated Press in April 2021: “You can’t pass it from one person to another if you stand next to someone.”
Centner Academy, a private school in Miami, Florida, announced in April 2021 that it would not employ vaccinated teachers, citing in a letter to parents anecdotal claims of women “reporting adverse reproductive issues from being in close proximity with those who have received any one of the COVID-19 injections.”
Dr. Aileen Marty, an infectious disease specialist with Florida International University, told WFOR, a CBS-owned TV station in Miami, after reviewing the Centner Academy letter: “There are no scientific bases for any of the concerns that they raise and there’s no foundation whatsoever. It shows me that the author has a very primitive understanding of what a vaccine is and really no understanding of the scientific process.”
-
MYTH: People vaccinated with COVID-19 vaccines can shed
disease-causing particles to others.
THE FACTS: In an April 2021 statement to Reuters, an unnamed U.S. Centers for Disease Control and Prevention spokesperson said, “There is no way for a COVID-19 vaccinated person to ‘shed vaccine.’ COVID-19 vaccines give instructions to teach our cells how to make a protein—or even just a piece of a protein—that triggers an immune response inside our bodies. After the protein piece is made, the cell breaks down the instructions and gets rid of them. The immune response, which produces antibodies, is what protects us from getting infected if the real virus enters our bodies.”
Only vaccines that contain a live virus can shed enough to potentially infect other people. USA Today reported in a May 2017 article that this occurred with the oral polio vaccine, which was distributed beginning in 1961, because children who received the vaccine shed the virus through their feces, and in rare cases, could be spread to others who didn’t wash their hands after using the bathroom.
The oral polio vaccine stopped being used in the U.S. by 2000, and Dr. Paul Offit, director of the Vaccine Education Center at the Children’s Hospital of Philadelphia, told USA Today that no other type of vaccine has ever been shown to shed in a manner that caused disease.
-
MYTH: The increase in COVID-19 cases and deaths in India between
February and May 2021 was caused by COVID-19 vaccinations.
THE FACTS: While the COVID-19 surge in India did begin after the country started administering COVID-19 vaccines on Jan. 16, 2021, the two events are not associated. Only 9.8 percent of the country’s population had received one dose of a COVID-19 vaccine as of May 10, 2021 — and the rate of vaccination was even lower when COVID-19 cases had begun to increase in February 2021, according to a May 2021 fact-checking article from Reuters.
According to Johns Hopkins University, India’s seven-day average of new COVID-19 cases went from a low of 11,145 on Feb. 11, 2021, to a peak of 391,232 on May 8, 2021.
Sumit Chanda, director of the immunity and pathogens program at Sanford Burnham Prebys Medical Discovery Institute in San Diego, California, told USA Today in May 2021, “There’s actually an inverse correlation between those people who got the vaccine and those people are getting sick,” meaning that vaccinated individuals were less likely to get COVID-19.
-
MYTH: Videos posted on social media show magnets sticking to
people’s arms after they received COVID-19 vaccines, proving the
vaccines contain magnetic ingredients.
THE FACTS: Dr. Stephen Schrantz, an infectious diseases specialist at the University of Chicago, called the videos “a hoax” in a May 2021 article by Agence France-Presse. “There is absolutely no way that a vaccine can lead to the reaction shown in these videos posted to Instagram and/or YouTube,” he said. “It is better explained by 2 sided tape on the metal disk being applied to the skin rather than a magnetic reaction.”
None of the COVID-19 vaccines authorized for widespread use in the U.S. and Europe contain magnetic ingredients or microchips. Lisa Morici, an associate professor at the Tulane University School of Medicine who studies vaccines, told FactCheck.org in May 2021 that the ingredients in the Pfizer, Moderna, and Johnson & Johnson COVID-19 vaccines “are simply RNA/DNA, lipids, proteins, salts, and sugars.”
Dr. Edward Hutchinson, a lecturer at the Centre for Virus Research at the University of Glasgow, told Newsweek in a May 2021 article that “you would need to introduce a large lump of magnetic material beneath the skin to get the action through the skin that the videos claim to show — if you want to give this a go, try getting a fridge magnet to pick up anything, particularly tiny bits of metal, through the skin between your thumb and index finger.”
-
MYTH: The American Red Cross will not accept blood donations from
anyone who has received a COVID-19 vaccine because the vaccines
wipe out the body’s natural antibodies.
THE FACTS: The American Red Cross accepts blood donations from people who have received a COVID-19 vaccine, according to its website. American Red Cross spokesperson Katie Wilkes told The Associated Press in May 2021, “In most cases, you can donate blood, platelets and plasma after a COVID-19 vaccine as long as you’re feeling healthy and well.”
Regarding the claim that the COVID-19 vaccines wipe out antibodies, Columbia University microbiology and immunology professor Vincent Racaniello told political site The Dispatch in May 2021, “Vaccines do just the opposite, they induce antibodies, not wipe them out. There are no data which would suggest that vaccines reduce antibody levels. Furthermore, if this were true, then there would be no blood supply as many people have received a variety of different vaccines.”
-
MYTH: Pfizer’s COVID-19 shot caused more deaths than the
AstraZeneca vaccine.
THE FACTS: There is no evidence of a causal link between the Pfizer-BioNTech COVID-19 vaccine and deaths among its recipients. Claims that the Pfizer vaccine is deadlier than other vaccines often cite unverified reports of deaths following vaccination, with no proof that the deaths were caused by the vaccine.
As of May 2021, the CDC said that it has not found any deaths directly related to the Pfizer COVID-19 vaccine. Multiple clinical trials and additional studies following emergency authorization have shown that the Pfizer vaccine is safe and effective at preventing symptomatic cases of COVID-19.
Several European news organizations, including French tech news site Numerama and German broadcaster Deutsche Welle, reported in May 2021 that a Russian-linked advertising agency attempted to run an anti-Pfizer disinformation campaign on social media, using similar arguments. French and German YouTubers and influencers said that an advertising agency called Fazze offered them money to post social media videos and messages warning against the Pfizer vaccine and claiming that “the death rate among the vaccinated with Pfizer is almost 3x higher than the vaccinated by AstraZeneca,” Numerama reported.
According to a May 2021 Wall Street Journal report, French counterintelligence authorities were investigating whether the Russian government was behind the Fazze emails and the related disinformation campaign. A 2021 report by the Alliance for Securing Democracy, an advocacy group that studies state disinformation, found that Russian state media outlets have repeatedly drawn unsubstantiated links between the Pfizer vaccine and deaths of vaccine recipients. Although it is not clear why Pfizer received such negative treatment by the Russians, the Alliance for Securing Democracy report notes that the Pfizer vaccine was the first Western vaccine to compete with the Russian state-backed Sputnik V vaccine.
-
MYTH: SM-102, an ingredient in Moderna’s COVID-19 vaccine, is
dangerous and has been listed as not being safe for human or
veterinary use by a company that sells the ingredient.
THE FACTS: SM-102 is a lipid, or a fatty molecule that is not soluble in water, which is used in Moderna’s COVID-19 vaccines to protect the messenger RNA that provides instructions to the body’s cells on creating antibodies against the COVID-19 virus, according to a May 2021 FactCheck.org article.
The claim that the ingredient is dangerous relied on misrepresenting a safety fact sheet from Michigan-based Cayman Chemical, which sells a SM-102 product as a “solution in chloroform,” a potentially toxic chemical that is not an ingredient in the Moderna vaccine.
The Cayman Chemical fact sheet does state that its SM-102 product is “not for human or veterinary diagnostic or therapeutic use.” However, its health warnings are related to the chloroform solution that makes up 90 percent of the product, not SM-102 itself. The fact sheet listed chloroform under “dangerous components,” while SM-102 is listed under “other ingredients.”
In a May 2021 press release, Cayman Chemical stated, “Neither the National Institute for Occupational Safety and Health (NIOSH), Registry of Toxic Effects of Chemical Substances (RTECS), or the European Chemicals Agency (ECHA) Classification and Labelling Inventory list any hazards associated with SM-102.”
-
MYTH: Denmark national soccer team player Christian Eriksen
received a COVID-19 vaccine days before he collapsed during a game
against Finland.
THE FACTS: Eriksen collapsed on the field during a June 12, 2021, match between Denmark and Finland, and went into cardiac arrest before being resuscitated. However, according to a June 2021 article from Reuters, Giuseppe Marotta, director of Eriksen’s club Inter Milan, told Italian sports TV channel Rai Sport, “He didn’t have COVID and wasn’t vaccinated either.”
PolitiFact reported in a June 2021 article that speculation that Eriksen’s collapse was connected to vaccines was fueled by Luboš Motl, a Czech physicist and blogger who has shared false claims about COVID-19 and vaccines. In a June 13, 2021, tweet, Motl claimed, “The chief medic and cardiologist of that Italian team confirmed on an Italian radio station that Eriksen has received the Pfizer vaccine on May 31.”
The official Twitter account for the Italian station, Radio Sportiva, denied that anyone from Inter Milan had confirmed Eriksen had been vaccinated on its station. In a June 13, 2021, tweet, the station said, “We have never reported any opinion from the Inter medical staff regarding Christian Eriksen’s condition. Please remove the content from the tweet author, otherwise we will be forced to take action.”
Correction: An earlier version of this report incorrectly listed the year a Reuters article about Christian Eriksen was published. It was 2021, not 2020. NewsGuard apologizes for the error.
-
MYTH: Gibraltar saw a surge in deaths since its government began
vaccinating the population with the Pfizer-BioNTech vaccine, with
at least 53 deaths caused by or linked to the COVID-19 vaccine in
Gibraltar.
THE FACTS: According to a January 2021 article from British fact-checking organization Full Fact, the figure of 53 deaths matched the total number of COVID-19 deaths reported in Gibraltar as of Jan. 20, 2021 — 10 days after COVID-19 vaccinations began in the British territory. However, there is no evidence linking those deaths to the COVID-19 vaccine.
In a Jan. 26, 2021, tweet, Fabian Picardo, the Chief Minister of Gibraltar, wrote “Do not believe this nonsense… I can tell you that we have had no deaths registered as arising from the vaccine.”
The Gibraltar government released a statement on its official website in January 2021 explaining that six people appeared to have contracted COVID-19 before they were vaccinated and died of causes unrelated to the vaccine.
“The Gibraltar Health Authority can confirm that there is no evidence that any of those 11,073 who have been vaccinated in Gibraltar have died as a result of any reaction to the vaccine,” the government’s statement said. “Statements to the contrary on social media are entirely untrue.”
-
MYTH: Four pilots who work for British Airways have died from the
COVID-19 vaccine, and now the airline is in “crisis talks” with
the British government about whether vaccinated pilots should be
allowed to fly.
THE FACTS: According to a June 2021 article from Reuters, British Airways confirmed that four pilots “had recently passed away.” However, the airline also told Reuters that there is no evidence the deaths were related to the COVID-19 vaccine. Additionally, the company said it was false that it was involved in any “crisis talks” with the British Government about its pilots.
The U.K. Medicines & Healthcare products Regulatory Agency, which operates the country’s Yellow Card Scheme to track adverse events following vaccinations, told Reuters in a statement, “We have not been made aware of deaths of BA pilots after receiving the Covid-19 vaccine and have not had discussions with BA or other airlines, about preventing pilots from flying after receiving the COVID-19 vaccine.”
-
MYTH: Airlines, particularly in Spain and Russia, have advised
people who have received the COVID-19 vaccine to avoid flying
because of a risk of developing blood clots.
THE FACTS: According to the U.S. Centers for Disease Control and Prevention, it is true that individuals with deep vein thrombosis (DVT) face a risk of blood clots from sitting for long periods of time on long flights. However, those clots are a different type than the rare complication attributed to the Johnson and Johnson or AstraZeneca COVID-19 vaccines. Blood clots from DVT typically occur in the legs, according to the CDC. Blood clots arising from Vaccine-induced Thrombosis and Thrombocytopenia (VITT) occurred elsewhere, such as in the brain or abdomen, according to an April 2021 study published in the New England Journal of Medicine.
“VITT is an immune reaction to vaccine[s] and is not provoked by flying,” Dr. Sue Pavord, Consultant Haematologist at Oxford University Hospitals and co-chair of the British Society for Hemaetology’s Obstetric Haematology Group, said in an email to Reuters in a June 2021 article. Moreover, Reuters reported that the International Air Transport Association (IATA), the trade association that represents 290 airlines worldwide, or 82 percent of the world’s total air traffic, said it was not aware of any airlines considering advising vaccinated individuals against flying.
Editor’s Note: This article was updated on Feb. 1, 2021, to include new information about the COVID-19 vaccines’ effectiveness against virus mutations.
The Top COVID-19 Vaccine Myths Spreading Online | Britannica
https://www.britannica.com/list/the-top-covid-19-vaccine-myths-spreading-online
Debunking mRNA Vaccine Misconceptions—An Overview for Medical Professionals
The hearts and minds of people worldwide have been consumed by the life-altering consequences of the Coronavirus disease 2019 (COVID-19) pandemic. Vaccine development is a cornerstone of the world's return to normalcy, and 2 mRNA-based vaccines have recently received Emergency Use Authorization from the Food and Drug Administration (FDA). Medical professionals have been offered these vaccines first due to their increased risk of infection with the novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) that causes COVID-19. Although work done at our University was instrumental in the development of mRNA vaccines,1 we have encountered, among some medical staff, a reluctance to receive the vaccine.
While logistical hurdles such as scheduling and availability may decrease vaccine utilization, a sizeable number of health care staff have expressed reservations about vaccination. One concern is that mRNA vaccine technology is new and long-term adverse effects in humans are unknown. Vaccines are traditionally composed of inactivated virus, live-attenuated virus, or antigenic proteins. Normally, mRNA is transcribed from DNA and is then translated to protein. mRNA has not been historically widely used as a vaccine due to the lability of RNA, which is typically rapidly degraded by ribonucleases. The Moderna and Pfizer/BioNTech COVID-19 vaccines that received Emergency Use Authorizations mitigate this and other problems via the use of modified mRNA and lipid nanoparticles (LNPs).
The use of modified mRNA may be a source of concern for some. Nucleosides are the building blocks of DNA and RNA. Previous work has demonstrated that substitution of the nucleoside uridine for pseudouridine or N1-methylpseudouridine enhances the stability of mRNA and decreases immunogenicity, so these nucleosides are used in both COVID-19 mRNA vaccines.2, 3, 4 Both of these modifications are naturally occurring in eukaryotic cells, thereby mitigating concerns of toxicity.
To mediate its therapeutic effect, the mRNA in the vaccine must traverse the cell membrane and be translated to protein; however, cellular uptake of mRNA is limited because it is anionic. LNPs encapsulate RNA and facilitate cellular entry. The use of LNPs and liposomes is not limited to mRNA vaccines. These compounds have already been used in FDA-approved chemotherapies, vaccines, antifungals, and analgesics.5
Although there are no previously approved mRNA vaccines, these vaccines have been trialed in humans for oncologic therapies for nearly a decade (NCT01684241), and have been trialed in humans for infectious disease for over 3 years.6 Regarding adverse events, data from phase I influenza mRNA vaccine and phase III COVID-19 mRNA vaccine trials have demonstrated that injection site pain, erythema, swelling, fever, fatigue, headache, chills, muscle pain, and arthralgia are more common in the vaccine group relative to placebo.3 , 4 , 6 These events are consistent with reactogenicity, which is expected after immune system instigation.
The COVID-19 phase III mRNA-LNP vaccine trials have monitored most subjects for more than 2 months, suggesting that long-term adverse effects are unlikely. Moderna has enrolled >1700 volunteers in 12 previous Phase I/II trials, and they have not reported any long-term adverse events.7 In the Moderna COVID-19 phase III vaccine trial data, the FDA did note an imbalance of cases of Bell's palsy in the vaccine group (n = 3) compared with the placebo group (n = 1). Only one case was ongoing; the rest were resolved or resolving.8 In the Pfizer/BioNTech trial, 4 cases of Bell's palsy were noted in the vaccine group and none in the placebo group. One case resolved and the others were continuing/resolving.9 This rate of Bell's palsy (0.02% for both trials) does not exceed the expected background rate of this disease. Furthermore, long-term adverse effects are unlikely mechanistically, because mRNA does not persist for an extended period of time or integrate into chromosomes.
Effective vaccines require an adequate immune response, so some vaccines include adjuvants to spur the immune system. While adjuvants have been utilized for decades, their mechanism of action is not entirely known. The Moderna and Pfizer/BioNTech COVID-19 mRNA vaccines stimulated a protective immune response with LNP acting as an adjuvant.2 This adjuvant is novel in that it specifically induces a CD4+ T cell helper response that stimulates antibody production, maturation, class switch, and long-term memory, known as T follicular helper cells.
Most who are reluctant to receive the vaccine cite safety concerns; however, some remain nihilistic about vaccine efficacy. The Pfizer/BioNTech vaccine demonstrated 95% efficacy and the Moderna vaccine showed similar efficacy as well.3 , 4 While the long-term durability of protection is not definitively known, booster doses could be given in the future if necessary. The SARS-CoV-2 virus, like other members of the coronavirus family, has the capacity to mutate and evolve. Indeed, new strains of the virus have been observed.10Although the virus has the capacity to mutate to evade our immune system, data have shown that an immune response to one strain of the virus can neutralize other viral strains.10 These data, coupled with the fact that immune responses to a vaccine will likely produce polyclonal antibodies, support efficacy of the vaccine despite viral mutations.
Another concern expressed by some is that the development and FDA review of the vaccines occurred too quickly for the vaccines to be adequately vetted. The development and review of these vaccines has been undeniably fast. The rapid development of the vaccines was possible due to the nature of mRNA vaccine production and the many years of preclinical and clinical development. All that is required for development is knowledge of the sequence of the antigen, in this case, the SARS-CoV-2 spike protein. Following their development, these vaccines underwent the same FDA review steps that all drugs are required to go through. The review process was quicker than normal due to the urgency of this pandemic. No steps were omitted in this process.
A greater understanding and acceptance of mRNA vaccines among the medical community is essential for widespread acceptance and utilization of these vaccines among our patients. In the rapidly evolving field of medicine, it is our collective responsibility to educate each other and our patients about novel therapeutics.
Footnotes
Funding: None.
Conflicts of Interest: None.
Authorship: Both authors have participated in the preparation of the manuscript.
References